Trigeminal nerve, n. trigeminus , mixed nerve. The motor fibers of the trigeminal nerve begin from its motor nucleus, which lies in the pons. The sensory fibers of this nerve approach the pontine nucleus, as well as the nuclei of the midbrain and spinal tract of the trigeminal nerve. This nerve innervates the skin of the face, frontal and temporal regions, the mucous membrane of the nasal cavity and paranasal sinuses, mouth, tongue (2/3), teeth, conjunctiva of the eye, masticatory muscles, muscles of the floor of the mouth (mylohyoid muscle and anterior belly of the biventricular muscles), as well as the muscles that strain the velum palatine and the tympanic membrane. In the area of all three branches of the trigeminal nerve there are vegetative (autonomous) nodes, which were formed from cells that moved out of the rhombencephalon during embryogenesis. These nodes are identical in structure to the intraorgan nodes of the parasympathetic part of the autonomic nervous system.
The trigeminal nerve exits the base of the brain with two roots (sensory and motor) at the point where the pons enters the middle cerebellar peduncle. Sensitive root radix sensoria, significantly thicker than the motor root, radix motoria. Next, the nerve goes forward and somewhat laterally, entering into the splitting of the dura mater of the brain - trigeminal cavity,cavum trigemi nale, lying in the area of the trigeminal depression on the anterior surface of the pyramid of the temporal bone. In this cavity there is a thickening of the trigeminal nerve - the trigeminal ganglion, gang lion trigeminale (Gasser knot). The trigeminal ganglion is crescent-shaped and is a cluster of pseudounipolar sensory nerve cells, the central processes of which form a sensory root and go to its sensory nuclei. The peripheral processes of these cells are sent as part of the branches of the trigeminal nerve and end with receptors in the skin, mucous membranes and other organs of the head. The motor root of the trigeminal nerve is adjacent to the trigeminal ganglion from below, and its fibers participate in the formation of the third branch of this nerve.
Three branches of the trigeminal nerve depart from the trigeminal ganglion: 1) the ophthalmic nerve (first branch); 2) maxillary nerve (second branch); 3) mandibular nerve (third branch). The ophthalmic and maxillary nerves are sensory, and the mandibular nerve is mixed, containing sensory and motor fibers. Each of the branches of the trigeminal nerve at its beginning gives off a sensitive branch to the dura mater of the brain.
optic nerve,P.ophthalmicus, departs from the trigeminal nerve in the area of its ganglion, is located in the thickness of the lateral wall of the cavernous sinus, and penetrates the orbit through the superior orbital fissure. Before entering the orbit, the optic nerve gives off tentorial (shell) branch, d.tentorii (meningeus). This branch goes posteriorly and branches in the tentorium of the cerebellum. In the orbit, the optic nerve is divided into the lacrimal, frontal and nasociliary nerves (Fig. 173).
1. Lacrimal nerve, P.lacrimdlis, runs along the lateral wall of the orbit to the lacrimal gland. Before entering the lacrimal gland, the nerve receives connecting branch, g.communications, cumP.zygomatico, connecting it with the zygomatic nerve (nerve of the second branch, P.trigeminus). This branch contains parasympathetic (postganglionic) fibers to innervate the lacrimal gland. The terminal branches of the lacrimal nerve innervate the skin and conjunctiva of the upper eyelid in the region of the lateral canthus. 2. Frontal nerve, P.frontalis, goes forward under the upper wall of the orbit, where it divides into two branches. One of its branches is supraorbital nerve, n.supraorbitalis, It leaves the orbit through the supraorbital notch and gives off medial and lateral branches, ending in the skin of the forehead. Second branch of the frontal nerve - supratrochlear nerve, n.supratrochledris, goes over the block of the superior oblique muscle and ends in the skin of the root of the nose, the lower part of the forehead, in the skin and conjunctiva of the upper eyelid, in the area of the medial corner of the eye. 3. Nasociliary nerve, P.nasocilia ris, is directed forward between the medial rectus and superior oblique muscles of the eye and gives off the following branches in the orbit: 1) front And posterior ethmoidal nerves, pp.ethmoiddles an terior et posterior, to the mucous membrane of the ethmoid sinuses and to the mucous membrane of the anterior part of the nasal cavity; 2) long ciliary branches, pp.ciliares longi, 2-4 branches go forward to the sclera and choroid eyeball;
3) subtrochlear nerve, n.infratrochledris, passes under the superior oblique muscle of the eye and goes to the skin of the medial corner of the eye and the root of the nose; 4) connecting branch (with ciliary node), d.communications (cum gdnglio cilidri), containing sensory nerve fibers, approaches the ciliary ganglion, which belongs to the parasympathetic part of the autonomic nervous system. Departing from the node 15-20 short ciliary nerves, pp.ciliares breves, heading to eyeball, carrying out its sensitive and autonomic innervation.
maxillary nerve,P.maxillaris, departs from the trigeminal ganglion, goes forward, exits the cranial cavity through the round foramen into the pterygopalatine fossa.
Even in the cranial cavity, they extend from the maxillary nerve meningeal (middle) branch, d.meningeus (medius), which accompanies the anterior branch of the middle meningeal artery and innervates the dura mater of the brain in the region of the middle cranial fossa. In the pterygopalatine fossa, the infraorbital and zygomatic nerves and nodal branches to the pterygopalatine ganglion depart from the maxillary nerve.
1Infraorbital nerve, P.infraorbitdlis, is a direct continuation of the maxillary nerve. Through the inferior orbital fissure, this nerve enters the orbit, passes first in the infraorbital groove and enters the infraorbital canal of the upper jaw. Coming from the canal through the infraorbital foramen to the anterior surface of the upper jaw, the nerve divides into several branches: 1) lower branches of the eyelids,rr. palpebrdles info- riores, directed to the skin of the lower eyelid; 2) external nasal branches,rr. nasdles externi, branch in the skin of the external nose; 3) superior labial branches,rr. labiates superiores. In addition, on its way, still in the infraorbital groove and in the canal, the infraorbital nerve gives off 4) superior alveolar nerves, n.alveoldres superiores, And anterior, middle and posterior alveolar branches,rr. alveoldres superiores anteriores, medius et posteridres, which in the thickness of the upper jaw form superior dental plexus,plexus dentdlis superior. Upper dental branchesrr. dentales superiores, this plexus innervates the teeth of the upper jaw, and upper gingival branches,rr. gingivdles superiores, - gums; 5) internal nasal branches,rr. nasdles interni, go to the mucous membrane of the anterior sections of the nasal cavity.
2Zygomatic nerve, P.zygomdticus, It arises from the maxillary nerve in the pterygopalatine fossa near the pterygopalatine ganglion and enters the orbit through the inferior orbital fissure. In the orbit, it gives off a connecting branch containing post-nodal parasympathetic fibers from the pterygopalatine ganglion to the lacrimal nerve for secretory innervation of the lacrimal gland. The zygomatic nerve then enters the zygomatic orbital foramen of the zygomatic bone. In the thickness of the bone, the nerve is divided into two branches, one of which is zygomaticotemporal branch, g.zygomaticotempordlis, exits through the opening of the same name into the temporal fossa and ends in the skin of the temporal region and the lateral corner of the eye. Another branch - zygomaticofacial, g.zygomaticofacidlis, through an opening on the anterior surface of the zygomatic bone it is directed to the skin of the zygomatic and cheek areas.
3 Nodal branches, rr. gangliondres [ ganglionici] , containing sensory fibers, go from the maxillary nerve (in the pterygopalatine fossa) to the pterygopalatine ganglion and to the branches extending from it.
Pterygopalatine ganglion, ganglion pterygopalatinum, refers to the parasympathetic part of the autonomic nervous system. This unit is suitable for: 1) nodal branches (sensitive- from the maxillary nerve), the fibers of which pass through the node in transit and are part of the branches of this node; 2) preganglionic parasympathetic fibers from the nerve of the pterygoid canal, which end in the pterygopalatine ganglion on the cells of the second neuron. The processes of these cells emerge from the node as part of its branches; 3) postganglionic sympathetic fibers from the nerve of the pterygoid canal, which pass through the node in transit and are part of the branches emerging from this node. Branches of the pterygopalatine ganglion:
1medial and lateral superior posterior nasal branches,rr. nasdles posteriores superiores middles et laterdles, penetrate through the sphenopalatine foramen and innervate the mucous membrane of the nasal cavity, including its glands. The largest of the superior medial branches is nasopalatine nerve, n.nasopala- tinus (nasopalatini), lies on the nasal septum, then is directed through the incisive canal to the mucous membrane of the hard palate;
2greater and lesser palatine nerves, p L palatinus major et tin. palatini minores, through the channels of the same name they follow to the mucous membrane of the hard and soft palate;
3inferior posterior nasal branches,rr. nasdles posteriores in- feriores, are branches of the greater palatine nerve, pass through the palatine canal and innervate the mucous membrane of the lower parts of the nasal cavity.
mandibular nerve,P.mandibuldris, exits the cranial cavity through the foramen ovale. It contains motor and sensory nerve fibers. When leaving the foramen ovale, motor branches depart from the mandibular nerve to the chewing muscles of the same name.
Motor branches: 1) masticatory nerve, n.mas- setericus; 2) deep temporal nerves, pp.tempordles profundi; 3) lateral and medial pterygoid nerves, pp.pterygoidei laterlis et medlis (Fig. 175); 4) nerve of the muscle that tenses the velum palatine, n.muscles tensoris veil palatini; 5) nerve of the tensor tympani muscle, n.muscles tensoris tympani.
Sensitive branches:
1Meningeal branch, G.meningeus, returns to the cranial cavity through the foramen spinosum (accompanies the middle meningeal artery) to innervate the dura mater of the brain in the region of the middle cranial fossa;
2Buccal nerve, ". buccdlis, first it goes between the heads of the lateral pterygoid muscle, then comes out from under the anterior edge of the masticatory muscle, lies on the outer surface of the buccal muscle, pierces it and ends in the mucous membrane of the cheek, as well as in the skin of the corner of the mouth.
3Auriculotemporal nerve, P.auriculotempordlis, begins with two roots that cover the middle meningeal artery, and then unite into one trunk. Having passed along the inner surface of the coronoid process of the mandible, the nerve bypasses its neck from behind and rises anteriorly from the cartilage of the external auditory canal, accompanying the superficial temporal artery. They arise from the auriculotemporal nerve anterior auricular nerves, pp.auriculars anteriores, to the front auricle; nerves of the external auditory canal, n.medtus acustici externi; branches of the eardrum,rr. Membrdnae tympani, to the eardrum; superficial temporal branches [nerves],rr. [ nn.] tempordles super fiddles, to the skin of the temporal region; parotid branches,rr. parotidei, containing postnodal parasympathetic secretory nerve fibers to the parotid salivary gland. These fibers joined the auriculotemporal nerve as part of connecting branch (with the auriculotemporal nerve), d.communications (cum n. auriculotempordlis).
81932 0
The ophthalmic nerve (n. ophthalmicus) is the first, thinnest branch of the trigeminal nerve. It is sensitive and innervates the skin of the forehead and the anterior part of the temporal and parietal regions, the upper eyelid, the back of the nose, as well as partially the mucous membrane of the nasal cavity, the membranes of the eyeball and the lacrimal gland (Fig. 1).
Rice. 1 . Nerves of the orbit, top view. (The levator muscle has been partially removed upper eyelid, and superior rectus and superior oblique muscles of the eye):
1 - long ciliary nerves; 2 - short ciliary nerves; 3, 11 - lacrimal nerve; 4 - ciliary node; 5 - oculomotor root of the ciliary ganglion; 6 - additional oculomotor root of the ciliary ganglion; 7 - nasociliary root of the ciliary node; 8 - branches of the oculomotor nerve to the inferior rectus muscle of the eye; 9, 14 - abducens nerve; 10 - lower branch of the oculomotor nerve; 12 - frontal nerve; 13 - optic nerve; 15 - oculomotor nerve; 16 - trochlear nerve; 17 - branch of the cavernous sympathetic plexus; 18 - nasociliary nerve; 19 - superior branch of the oculomotor nerve; 20 - posterior ethmoidal nerve; 21 - optic nerve; 22 - anterior ethmoidal nerve; 23 - subtrochlear nerve; 24 - supraorbital nerve; 25 - supratrochlear nerve
The nerve is 2-3 mm thick, consists of 30-70 relatively small bundles and contains from 20,000 to 54,000 myelinated nerve fibers, mostly of small diameter (up to 5 microns). After originating from the trigeminal ganglion, the nerve passes through the outer wall of the cavernous sinus, where it gives off recurrent shell (tentorial) branch (r. meningeus recurrens (tentorius) to the tentorium of the cerebellum. Near the superior orbital fissure, the optic nerve divides into 3 branches: lacrimal, frontal and theoretical nerves.
1. Lacrimal nerve (p. lacrimalis) is located near the outer wall of the orbit, where it receives connecting branch with the zygomatic nerve (r. communicant cum nervo zygomatico). Provides sensitive innervation to the lacrimal gland, as well as the skin of the upper eyelid and lateral canthus.
2. The frontal nerve (p. frontalis) is the thickest branch of the optic nerve. It passes under the upper wall of the orbit and divides into two branches: supraorbital nerve(n. supraorbitalis), going through the supraorbital notch to the skin of the forehead, and supratrochlear nerve(n. supratrochlearis), emerging from the orbit at its inner wall and innervating the skin of the upper eyelid and medial corner of the eye.
3. Nasociliary nerve(p. nasociliaris) lies in the orbit at its medial wall and, under the block of the superior oblique muscle, exits the orbit in the form of a terminal branch - subtrochlear nerve(p. infratrochlearis), which innervates the lacrimal sac, conjunctiva and medial corner of the eye. Along its length, the nasociliary nerve gives off the following branches:
1) long ciliary nerves (pp. ciliares longi) to the eyeball;
2) posterior ethmoidal nerve (p. ethmoidalis posterior) to the mucous membrane of the sphenoid sinus and the posterior cells of the ethmoidal labyrinth;
3) anterior ethmoidal nerve (n. ethmoidalis anterior) to the mucous membrane frontal sinus and nasal cavity ( rr. nasales interni laterales et mediates) and to the skin of the tip and wing of the nose.
In addition, a connecting branch departs from the nasociliary nerve to the ciliary ganglion.
(ganglion ciliare) (Fig. 2), up to 4 mm long, lies on the lateral surface of the optic nerve, approximately on the border between the posterior and middle thirds of the length of the orbit. In the ciliary ganglion, as in other parasympathetic ganglia of the trigeminal nerve, there are parasympathetic multi-process (multipolar) nerve cells on which preganglionic fibers, forming synapses, switch to postganglionic ones. Sensitive fibers pass through the node in transit.

Rice. 2. Ciliary node (preparation by A.G. Tsybulkin). Impregnation with silver nitrate, clearing in glycerin. Uv. x12.
1 - ciliary node; 2 - branch of the oculomotor nerve to the inferior oblique muscle of the eye; 3 - short ciliary nerves; 4 - ophthalmic artery; 5 - nasociliary root of the ciliary node; 6 - accessory oculomotor roots of the ciliary ganglion; 7 - oculomotor root of the ciliary ganglion
Connecting branches in the form of its roots approach the node:
1) parasympathetic (radix parasympathica (oculomotoria) gangliiciliaris)- from the oculomotor nerve;
2) sensitive (radix sensorial (nasociliaris) ganglii ciliaris)- from the nasociliary nerve.
From the ciliary node extends from 4 to 40 short ciliary nerves (pp. ciliares breves), going inside the eyeball. They contain postganglionic parasympathetic fibers innervating the ciliary muscle, sphincter and, to a lesser extent, the pupillary dilator, as well as sensory fibers to the membranes of the eyeball. (Sympathetic fibers to the dilator muscle are described below.)
(n. maxillaries) - the second branch of the trigeminal nerve, sensitive. It has a thickness of 2.5-4.5 mm and consists of 25-70 small bundles containing from 30,000 to 80,000 myelinated nerve fibers, mostly of small diameter (up to 5 microns).
The maxillary nerve innervates the dura mater of the brain, the skin of the lower eyelid, the lateral corner of the eye, the anterior temporal region, the upper part of the cheek, the wings of the nose, skin and mucous membrane upper lip, mucous membrane of the posterior and lower parts of the nasal cavity, mucous membrane of the sphenoid sinus, palate, teeth of the upper jaw. Upon exiting the skull through the foramen rotundum, the nerve enters the pterygopalatine fossa, passes from back to front and from the inside to the outside (Fig. 3). The length of the segment and its position in the fossa depend on the shape of the skull. In a brachycephalic skull, the length of the nerve segment in the fossa is 15-22 mm, it is located deep in the fossa - up to 5 cm from the middle of the zygomatic arch. Sometimes the nerve in the pterygopalatine fossa is covered by a bone crest. In a dolichocephalic skull, the length of the nerve section in question is 10-15 mm, it is located more superficially - up to 4 cm from the middle of the zygomatic arch.

Rice. 3. Maxillary nerve, lateral view. (The wall and contents of the orbit have been removed):
1 - lacrimal gland; 2 - zygomaticotemporal nerve; 3 - zygomaticofacial nerve; 4 - external nasal branches of the anterior ethmoidal nerve; 5 - nasal branch; 6 - infraorbital nerve; 7 - anterior superior alveolar nerves; 8 - mucous membrane of the maxillary sinus; 9 - middle superior alveolar nerve; 10—dental and gingival branches; 11 - upper dental plexus; 12—infraorbital nerve in the canal of the same name; 13 - posterior superior alveolar nerves: 14 - nodal branches to the pterygopalatine node; 15 - greater and lesser palatine nerves: 16 - pterygopalatine ganglion; 17 - nerve of the pterygoid canal; 18 - zygomatic nerve; 19 - maxillary nerve; 20 - mandibular nerve; 21 - foramen ovale; 22 - round hole; 23 - meningeal branch; 24 - trigeminal nerve; 25 - trigeminal node; 26 - optic nerve; 27 - frontal nerve; 28 - nasociliary nerve; 29 - lacrimal nerve; 30 - ciliary node
Within the pterygopalatine fossa, the maxillary nerve gives off meningeal branch (g. meningeus) to the dura mater and divides into 3 branches:
1) nodal branches to the pterygopalatine node;
2) zygomatic nerve;
3) the infraorbital nerve, which is a direct continuation of the maxillary nerve.
1. Nodal branches to the pterygopalatine ganglion (rr. ganglionares ad ganglio pterygopalatinum) (1-7 in number) depart from the maxillary nerve at a distance of 1.0-2.5 mm from the foramen rotundum and go to the pterygopalatine ganglion, giving sensory fibers to the nerves starting from the ganglion. Some nodal branches bypass the node and join its branches.
Pterygopalatine ganglion(ganglion pterygopalatinum) - formation of the parasympathetic part of the autonomic nervous system. The node is triangular in shape, 3-5 mm long, contains multipolar cells and has 3 roots:
1) sensitive - nodal branches;
2) parasympathetic - greater petrosal nerve(n. petrosus major)(branch of the intermediate nerve), contains fibers to the glands of the nasal cavity, palate, lacrimal gland;
3) sympathetic - deep petrosal nerve(n. petrosus profundus) originates from the internal carotid plexus and contains post-ganglionic sympathetic nerve fibers from the cervical ganglia. As a rule, the large and deep petrosal nerves unite into the nerve of the pterygoid canal, which passes through the canal of the same name at the base of the pterygoid process of the sphenoid bone.
Branches extend from the node, which include secretory and vascular (parasympathetic and sympathetic) and sensory fibers (Fig. 4):

Rice. 4. Pterygopalatine ganglion (diagram):
1 - superior salivary nucleus; 2—facial nerve; 3— genu of the facial nerve; 4 - greater petrosal nerve; 5— deep petrosal nerve; 6— nerve of the pterygoid canal; 7 - maxillary nerve; 8— pterygopalatine node; 9 - posterior superior nasal branches; 10—infraorbital nerve; 11 - nasopalatine nerve; 12 - postganglionic autonomic fibers to the mucous membrane of the nasal cavity; 13 - maxillary sinus; 14 - posterior superior alveolar nerves; 15—greater and lesser palatine nerves; 16—tympanic cavity; 17— internal carotid nerve; 18— internal carotid artery; 19—top cervical node sympathetic trunk; 20 - autonomous nuclei of the spinal cord; 21 - sympathetic trunk; 22 - spinal cord; 23 - medulla oblongata
1) orbital branches(rr. orbitales), 2-3 thin trunks, penetrate through the inferior orbital fissure and then, together with the posterior ethmoidal nerve, go through the small openings of the sphenoid-ethmoidal suture to the mucous membrane of the posterior cells of the ethmoidal labyrinth and the sphenoid sinus;
2) posterior superior nasal branches(rr. nasales posteriores superiors)(8-14 in number) exit the pterygopalatine fossa through the sphenopalatine foramen into the nasal cavity and are divided into two groups: lateral and medial (Fig. 5). Lateral branches (rr. nasales posteriores superiores laterales)(6-10), go to the mucous membrane of the posterior sections of the superior and middle nasal concha and nasal passages, the posterior cells of the ethmoid bone, the upper surface of the choanae and the pharyngeal opening of the auditory tube. Medial branches (rr. nasales posteriores superiores mediates)(2-3), branch in the mucous membrane upper section nasal septum.

Rice. 5. Nasal branches of the pterygopalatine ganglion, view from the nasal cavity: 1 - olfactory filaments; 2, 9 - nasopalatine nerve in the incisive canal; 3 - posterior superior medial nasal branches of the pterygopalatine ganglion; 4 - posterior superior lateral nasal branches; 5 - pterygopalatine node; 6 - posterior lower nasal branches; 7 - lesser palatine nerve; 8 - greater palatine nerve; 10 - nasal branches of the anterior ethmoidal nerve
One of the medial branches is nasopalatine nerve (n. nasopalatinus)- passes between the periosteum and the mucous membrane of the septum along with posterior artery the nasal septum forward, to the nasal opening of the incisive canal, through which it reaches the mucous membrane of the anterior part of the palate (Fig. 6). Forms a connection with the nasal branch of the superior alveolar nerve.

Rice. 6. Sources of innervation of the palate, ventral view (soft tissues removed):
1 - nasopalatine nerve; 2 - greater palatine nerve; 3 - lesser palatine nerve; 4 - soft palate
3) palatine nerves (pp. palatine) spread from the node through the greater palatine canal, forming 3 groups of nerves:
1) greater palatine nerve (p. palatinus major)- the thickest branch, exits through the large palatine foramen onto the palate, where it splits into 3-4 branches that innervate most mucous membrane of the palate and its glands in the area from the fangs to soft palate;
2)minor palatine nerves (par. palatini minores) enter the oral cavity through the small palatine openings and branch in the mucous membrane of the soft palate and the region of the palatine tonsil;
3) lower posterior nasal branches (rr. nasales posteriores inferiors) They enter the greater palatine canal, leave it through small openings and, at the level of the inferior turbinate, enter the nasal cavity, innervating the mucous membrane of the inferior turbinate, middle and lower nasal passages and the maxillary sinus.
2. The zygomatic nerve (n. zygomaticus) branches off from the maxillary nerve within the pterygopalatine fossa and penetrates through the inferior orbital fissure into the orbit, where it runs along the outer wall, gives off a connecting branch to the lacrimal nerve, containing secretory parasympathetic fibers to the lacrimal gland, enters into the zygomaticoorbital foramen and inside the zygomatic bone it is divided into two branches:
1) zygomaticofacial branch(g. zygomaticofacialis), which exits through the zygomatic-facial foramen onto the anterior surface of the zygomatic bone; in the skin of the upper part of the cheek it gives off a branch to the area of the outer canthus and a connecting branch to the facial nerve;
2) zygomaticotemporal branch(g. zygomaticotemporalis), which leaves the orbit through the opening of the zygomatic bone of the same name, pierces the temporalis muscle and its fascia and innervates the skin of the anterior part of the temporal and posterior part of the frontal regions.
3. Infraorbital nerve(n. infraorbitalis) is a continuation of the maxillary nerve and gets its name after the above branches depart from it. The infraorbital nerve leaves the pterygopalatine fossa through the inferior orbital fissure, passes along the lower wall of the orbit along with the vessels of the same name in the infraorbital groove (in 15% of cases there is a bone canal instead of a groove) and exits through the infraorbital foramen under the muscle that lifts the upper lip, dividing into terminal branches. The length of the infraorbital nerve is different: with brachycephaly, the nerve trunk is 20-27 mm, and with dolichocephaly - 27-32 mm. The position of the nerve in the orbit corresponds to the parasagittal plane drawn through the infraorbital foramen.
The origin of the branches can also be different: scattered, in which numerous thin nerves with many connections depart from the trunk, or mainline with a small number of large nerves. Along its path, the infraorbital nerve gives off the following branches:
1) superior alveolar nerves(pp. alveolares superiors) innervate the teeth and upper jaw (see Fig. 4). There are 3 groups of branches of the superior alveolar nerves:
1) posterior superior alveolar branches (rr. alveolares superiores posteriors) They branch from the infraorbital nerve, as a rule, in the pterygopalatine fossa, numbering 4-8 and located together with the vessels of the same name along the surface of the tubercle of the upper jaw. Some of the most posterior nerves go along the outer surface of the tubercle down to the alveolar process, the rest enter through the posterior superior alveolar foramina into the alveolar canals. Branching together with other superior alveolar branches, they form the nervous superior dental plexus(plexus dentalis superior), which lies in the alveolar process of the upper jaw above the apexes of the roots. The plexus is dense, broadly looped, stretched along the entire length of the alveolar process. They depart from the plexus upper gingival branches (rr. gingivales superiors) to the periodontium and periodontium in the area of the upper molars and upper dental branches (rr. dentales superiors)- to the tips of the roots of large molars, in the pulp cavity of which they branch. In addition, the posterior superior alveolar branches send thin nerves to the mucous membrane of the maxillary sinus;
2) middle superior alveolar branch (r. alveolaris superior) in the form of one or (less often) two trunks it branches off from the infraorbital nerve, most often in the pterygopalatine fossa and (less often) within the orbit, passes in one of the alveolar canals and branches in the bone canaliculi of the upper jaw as part of the superior dental plexus. It has connecting branches with the posterior and anterior superior alveolar branches. Innervates the periodontium and periodontium in the area of the upper premolars through the upper gingival branches and the upper premolars through the upper dental branches;
3) anterior superior alveolar branches (rr. alveolares superiores ateriores) arise from the infraorbital nerve in the anterior part of the orbit, which leaves through the alveolar canals, penetrating the anterior wall of the maxillary sinus, where they form part of the superior dental plexus. Upper gingival branches innervate the mucous membrane of the alveolar process and the walls of the alveoli in the area of the upper canines and incisors, upper dental branches- upper canines and incisors. The anterior superior alveolar branches send a thin nasal branch to the mucous membrane of the anterior floor of the nasal cavity;
2) lower branches of the eyelids(rr. palpebrales inferiors) they branch from the infraorbital nerve as they exit the infraorbital foramen, penetrate through the levator labii superioris muscle, and, branching, innervate the skin of the lower eyelid;
3) external nasal branches(rr. nasales superiors) innervate the skin in the area of the wing of the nose;
4) internal nasal branches(rr. nasales interni) approach the mucous membrane of the vestibule of the nasal cavity;
5) superior labial branches(rr. labiates superiors)(3-4 in number) go down between the upper jaw and the muscle that lifts the upper lip; innervate the skin and mucous membrane of the upper lip to the corner of the mouth.
All of the listed external branches of the infraorbital nerve form connections with the branches of the facial nerve.
Human anatomy S.S. Mikhailov, A.V. Chukbar, A.G. Tsybulkin
Our nervous system is usually divided into several sections. They distinguish, and everyone knows this from the school curriculum, into a central and a peripheral department. The autonomic nervous system is distinguished separately. Central department- this is nothing more than the spinal cord and brain. Peripheral part directly connected to the central part nervous system(CNS), represented by the spinal and cranial nerves. They also transmit various kinds of “information” to the central nervous system from receptors located in different parts our body.
Location of cranial nerves, ventral view
In total there are 12 of them or sometimes 13. Why sometimes thirteen? The fact is that only some of the authors call one of them, the intermediate one, the 13th pair.
More about the trigeminal nerve
The fifth, one of the largest, pair of cranial nerves, namely (trigeminal nerve - nervus trigeminus). Let us dwell in more detail on the anatomy and diagram of the trigeminal nerve. Its fibers originate in the nuclei of the brain stem. In this case, the nuclei are located in the projection of the bottom of the fourth ventricle. To more accurately understand where the trigeminal nerve is located in humans, see the photo.
Exit point and location of the main branches of the trigeminal nerve
General structure
The nervus trigeminus itself is mixed, that is, it carries motor (motor) and sensitive (sensory) fibers. Motor fibers transmit information from muscle cells(myocytes), and sensory ones “serve” various receptors. The trigeminal facial nerve exits the brain just in the area where the pons and middle cerebellar peduncle converge. And it immediately “forks out.”
Main branches
Imagine a tree branch from which thinner branches diverge in different directions. Introduced? The same goes for the trigeminal nerve. In the anatomy of the trigeminal nerve, its branches also diverge to the sides with many branches. There are three branches in total:
main branches of the trigeminal nerve and areas of their innervation
Ophthalmic branch
The ophthalmic (Latin name is nervus ophtalmicus) is the first (1) branch of the trigeminal nerve (in the photo the uppermost). Entirely composed of sensory fibers. This means that it only transmits data from different receptors. For example, receptors for tactile, temperature, pain sensitivity. If we continue the analogy with the tree, the optic nerve also branches, only this happens in the orbit. Thus, the superior orbital fissure (n.ophthalmicus enters the orbit through it) is one of the points of exit of the trigeminal nerve from the cranial cavity. Surprisingly, n.ophthalmicus also branches into several branches:
- frontal - the longest.
- the lacrimal gland, which passes between the muscles responsible for eye movements and innervates the lacrimal gland.
- nasociliary, it is she who innervates our eyelashes and part of the nasal epithelium.
Maxillary branch
Maxillary (Latin name - nervus maxillaris) - second (2) branch. Sensory, that is, it also consists of one hundred percent sensory fibers. It branches in the orbit, however, it gets there not through the upper, but through the lower orbital fissure (it becomes the second exit point from the cranial cavity, where the ternary nerve is located along with the nuclei). Let's look at the branches of the maxillary nerve. An important part, which is a network of fibers extending from n. maxillaris is the upper dental plexus, as the name implies, its function is to provide communication between the central nervous system and receptors located in the gums and teeth. As soon as the maxillary nerve passes into the infraorbital groove, it becomes infraorbital. The zone of its innervation becomes clear from the names of its small branches: external nasal, upper labial, lower branches of the eyelids. The zygomatic nerve is the only branch of the maxillary nerve that separates from the latter outside the orbit. But then it still penetrates into the orbit, however, not through the lower, but through the upper orbital fissure. And it innervates mainly the skin of the face, in the area adjacent to the cheekbones, as the name implies.
Mandibular branch
The mandibular (Latin name is nervus mandibularis) is the third (3) branch of the trigeminal nerve. The sensory-motor branch, unlike the two previous branches, is mixed and contains sensory and motor fibers. She is the largest. It exits the skull near the foramen magnum, through the foramen ovale. Upon exiting, it almost immediately branches into several branches.
Sensory (sensory) branches of the mandibular nerve:
- Lower alveolar (Latin name - nervus alveolaric inferior) - remember just above we talked about the upper dental plexus? So, there is also a lower one, it is formed precisely from the fibers of this branch of the n.mandibularis. That's right, because the lower teeth and gums cannot remain without innervation, right?
- Buccal (Latin name n. buccalis) - passes through the buccal muscle and approaches the epithelium of the cheek.
- Lingual (Latin name - nervus lingualis) - its “coverage area” becomes, as the name suggests, the mucous membrane of the tongue, and not all of it, but only 60 - 70%, located towards the front.
- The meningeal branch (Latin name ramus meningeus) - makes a 180-degree turn and approaches the dura mater, and for this it returns to the cranial cavity.
- Auricular-temporal (Latin name nervus auriculotemporalis) - carries information from the ear and the “adjacent territory”, the auricle along with the ear canal, the skin in the temple area
Motor fibers of the n.mandibularis (mandibular nerve):
- The chewing branch is needed so that the chewing muscles contract in time when we see some tasty food.
- The deep temporal branches are generally needed for the same thing, only they innervate slightly different masticatory muscles.
- The pterygoid branches (there are two of them, lateral and medial) also innervate several other muscles needed for chewing.
Trigeminal neuralgia is a fairly common disease of the peripheral nervous system, the main symptom of which is paroxysmal, very intense pain in the area of innervation (connection with the central nervous system) of one of the branches of the trigeminal nerve.
Trigeminal neuralgia does not go away painlessly; it is a rather serious illness. This disease most often affects women aged 50-70 years. In some cases, even surgery is required.
The trigeminal nerve originates from the trunk of the anterior part of the pons, located next to the middle cerebellar peduncles. It is formed from two roots - a large sensory root and a small motor one. Both roots from the base are directed to the apex of the temporal bone.
The motor root, together with the third sensory branch, exits through the foramen ovale and further connects with it. In the depression at the level of the upper part of the pyramidal bone there is a semilunar node. Three main sensory branches of the trigeminal nerve emerge from it (see photo).

Neuralgia in translation means pain along the nerve. Having 3 branches, the trigeminal nerve is responsible for the sensitivity of one side of the face and innervates strictly defined areas:
- 1 branch - orbital region;
- 2nd branch - cheek, nostril, upper lip and gum;
- 3rd branch - lower jaw, lip and gum.
All of them, on their way to the innervated structures, pass through certain openings and channels in the bones of the skull, where they can be subjected to compression or irritation. Neuralgia of the 1st branch of the trigeminal nerve is extremely rare; most often the 2nd and/or 3rd branches are affected.
If one of the branches of the trigeminal nerve is affected, a variety of disorders may occur. For example, the area of innervation may become insensitive. Sometimes, on the contrary, it becomes too sensitive, almost to the point of being painful. Often part of the face seems to sag or becomes less mobile.
Conventionally, all types of trigeminal neuralgia can be divided into primary (true) and secondary neuralgia.
- Primary (true) neuralgia is considered a separate pathology that occurs as a result of compression of the nerve or impaired blood supply in this area.
- Secondary neuralgia is the result of other pathologies. These include tumor processes, severe infectious diseases.
Causes
The exact cause of the development of trigeminal neuralgia is not clear; as mentioned above, it is an idiopathic disease. But there are factors that most often lead to the development of this disease.
The reasons for the development of trigeminal neuralgia are varied:
- compression of the nerve in the area of its exit from the cranial cavity through the bone canal with an abnormal arrangement of cerebral vessels;
- aneurysm of a vessel in the cranial cavity;
- metabolic disorder: gout, diabetes, thyroid diseases and other endocrine pathologies;
- hypothermia of the face;
- chronic infectious diseases in the facial area (chronic sinusitis, dental caries);
- metabolic disorders (diabetes mellitus, gout);
- chronic infectious diseases (tuberculosis, brucellosis, syphilis, herpes);
- mental disorders;
- suppuration of the bones of the skull, especially the jaws (osteomyelitis);
- severe allergic diseases;
- helminthiases (worms);
- multiple sclerosis;
- brain tumors.
Symptoms of trigeminal neuralgia
The disease is more typical for middle-aged people, most often diagnosed at 40-50 years of age. Females suffer more often than males. Damage to the right trigeminal nerve is most often observed (70% of all cases of the disease). Very rarely, trigeminal neuralgia can be bilateral. The disease is cyclical, that is, periods of exacerbation are followed by periods of remission. Exacerbations are more typical in the autumn-spring period.
So, typical signs of pain syndrome with trigeminal neuralgia:
- the nature of the pain in the face is shooting, extremely hard; patients often compare it to an electric shock
- duration of an attack of neuralgia - 10-15 seconds (no more than two minutes)
- the presence of a refractory period (the interval between attacks)
- localization of pain - does not change for several years
- pain of a certain direction (from one part of the face goes to another)
- the presence of trigger zones (areas of the face or oral cavity, irritation of which causes a typical paroxysm)
- the presence of trigger factors (actions or conditions under which a painful attack occurs; for example, chewing, washing, talking)
- The characteristic behavior of the patient during an attack is the absence of crying, screaming and a minimum of movements.
- twitching of the chewing or facial muscles at the peak of a painful attack.
From secondary symptoms Trigeminal neuralgia should be distinguished as phobic syndrome. It is formed against the background of “protective behavior,” when a person avoids certain movements and postures so as not to provoke an exacerbation of the disease.
- Chewing food with the side opposite the painful side;
- Neuropathic complications of neuralgia lead to secondary pain in the head;
- Concomitant irritation of the auditory and facial nerves.
Symptoms are difficult to interpret correctly if pain syndrome expressed slightly in the patient.
Due to the fact that all patients suffering from trigeminal neuralgia use only the healthy half of the mouth for chewing, muscle compactions form on the opposite side. With a long course of the disease, dystrophic changes in the masticatory muscles and a decrease in sensitivity on the affected side of the face may develop.
Localization of pain
Painful attacks may not be isolated, but follow each other at short intervals. The pathogenesis of the development of trigeminal neuralgia is very diverse:
- Usually, unpleasant sensations in any part of the face manifest themselves in the form of an attack.
- The pain numbs the person for a couple of minutes and temporarily subsides. Then he comes again. Between painful attacks it takes from 5 minutes to an hour.
- The defeat is reminiscent of being hit with a stun gun. Discomfort is usually localized in one part of the face, but often the patient feels pain in several places at once.
- It seems to a person that the pain covers the entire head, eye area, ears, nose. It is very difficult to speak during an attack.
- The pain that cramps the oral cavity makes it extremely difficult to pronounce words. This may cause severe muscle twitching.
Other diseases are similar to the symptoms of trigeminal neuralgia. These include temporal tendonitis, Ernest's syndrome and occipital neuralgia. With temporal tendonitis, the pain involves the cheek and teeth, observed headache and pain in the neck.
With occipital neuralgia, pain is usually located in front and behind the head and can sometimes spread to the face.
What most often causes pain in trigeminal neuralgia?
If the patient has neuralgia, then each attack occurs due to irritation of the trigeminal nerve, due to the existence of trigger, or “trigger” zones. They are localized on the face: in the corners of the nose, eyes, nasolabial folds. With irritation, sometimes extremely weak, they can begin to “generate” a stable, long-lasting painful impulse.
Factors causing pain may be:
- shaving procedure for men. Therefore, the appearance of a patient with a shaggy beard may lead an experienced doctor to “experienced neuralgia”;
- just a light stroke of the face. Such patients protect their face very carefully and do not use a handkerchief or napkin.
- the process of eating, the procedure of brushing teeth. Muscle movements oral cavity, cheek muscles and constrictors of the pharynx provoke pain as the facial skin begins to shift;
- fluid intake process. One of the painful conditions, since quenching thirst is punished by severe pain;
- an ordinary smile, as well as crying and laughing, talking;
- applying makeup to the face;
- sensation of pungent odors, which are called “trigeminal” - acetone, ammonia.
Consequences of neuralgia for humans
Trigeminal neuralgia in an advanced state entails certain consequences:
- paresis of facial muscles;
- hearing impairment;
- paralysis of facial muscles;
- development of facial asymmetry;
- prolonged pain;
- damage to the nervous system.
The risk group consists of older people (usually women), people suffering from cardiovascular diseases or metabolic disorders.
Diagnostics
A neurologist needs to differentiate frontal sinusitis, glaucoma, dental diseases, otitis, mumps, ethmoiditis or sinusitis. For this, a comprehensive examination is prescribed.
Typically, the diagnosis of trigeminal neuralgia is made based on the patient’s complaints and examination. Magnetic resonance imaging is important in diagnosing the cause of neuralgia. It allows you to identify a tumor or signs of multiple sclerosis.
Basic diagnostic methods:
- Consultation with a neurologist. Based on the results of the initial examination, the doctor determines further types of examination.
- Dental examination. Neuralgia often occurs against the background of dental diseases and poor-quality dentures.
- Panoramic x-ray of the skull and teeth. Helps to see formations that could be pinching a nerve.
- MRI. The study helps to see the structure of nerves, presence and location vascular pathologies, various types of tumors.
- Electromyography is designed to study the characteristics of the passage of impulses along a nerve.
- Blood test - allows you to exclude the viral origin of pathological changes in the trigeminal nerve.
If you have been diagnosed with neuralgia, do not be alarmed; in general, the prognosis is favorable, but timely treatment plays an important role.
Treatment of trigeminal neuralgia
It is extremely difficult to cure this disease and even radical treatment methods do not always provide positive result. But proper therapy can relieve pain and significantly alleviate human suffering.

The main treatment methods for trigeminal neuralgia include:
- medicinal;
- physiotherapy;
- surgical treatment.
Medications
Various groups of drugs are used in drug treatment, including:
- Anticonvulsants
- Antispasmodics and muscle relaxants.
Before using any drug, consultation with a neurologist is necessary.
Finlepsin for trigeminal neuralgia is one of the most common anticonvulsants. Active ingredient This drug is carbamazepine. This drug plays the role of an analgesic for idiopathic neuralgia or a disease that occurs against the background of multiple sclerosis.
In patients with trigeminal neuralgia, Finlepsin stops the onset of pain attacks. The effect is noticeable 8 to 72 hours after taking the drug. The dosage is selected only by the doctor individually for each patient.
The dose of Finlepsin (carbamazepine), with which patients can talk and chew painlessly, should remain unchanged for a month, after which it should be gradually reduced. Therapy with this drug can last until the patient notes the absence of attacks for six months.
Other drugs for trigeminal neuralgia:
- Gabapentin;
- Baclofen;
- Valproic acid;
- Lamotrigine;
- Pregabalin.
Each of these drugs has indications for use in trigeminal neuralgia. Sometimes these drugs do not help, so phenytoin is prescribed at a dose of 250 mg. The drug has a cardiodepressive effect, so it should be administered slowly.
Physiotherapeutic procedures
Physiotherapeutic procedures include paraffin baths, application different types currents, acupuncture. To get rid of severe pain, doctors give the patient alcohol-novocaine blockades. This is enough for some time, but the blockades are less and less effective each time.
- The following methods are used:
- Acupuncture;
- Magnetotherapy;
- Ultrasound;
- Laser treatment;
- Electrophoresis with drugs.
Surgical treatment of trigeminal neuralgia
During surgical treatment, the doctor tries to eliminate the compression of the nerve trunk by the blood vessel. In other cases, the trigeminal nerve itself or its node is destroyed in order to relieve pain.
Surgical treatments for trigeminal neuralgia are often minimally invasive. In addition, the surgical method also includes the so-called. Radiosurgery is a bloodless intervention that does not require any incisions or stitches.
There are the following types of operations:
- Percutaneous surgery. Apply on early stages diseases. Under local anesthesia The trigeminal nerve is destroyed by exposing it to chemicals or radio waves.
- Nerve decompression. This operation is aimed at correcting the location of the arteries that compress the trigeminal nerve.
- Radiofrequency destruction of the nerve root. In this operation, only a certain part of the nerve is destroyed.
The type of operation is prescribed depending on the individual characteristics of the patient’s disease.
A characteristic feature of all surgical methods The effect is more pronounced when they are carried out early. Those. The earlier this or that operation is performed, the higher the likelihood of cure.
Folk remedies for use at home
How to treat neuralgia with folk remedies? Using folk remedies It is important to remember that only symptoms are relieved in this way. Of course, first of all, you should use folk recipes that can effectively help fight the inflammatory process.
It is important to remember that the use of a particular treatment method should be discussed with a doctor. Pay attention to the consequences that drug treatment may bring.
Folk remedies for treating neuralgia at home:
- Birch juice. By taking it orally or lubricating it on the side of the face affected by neuralgia, you can reduce the symptoms of the disease. You need to drink 4-5 glasses of this juice per day.
- The beets are grated on a coarse grater. A small envelope is made from the bandage (the bandage is rolled up in several layers), into which the grated beets are placed. Such a bundle is inserted into the ear canal from the side where the inflammation appears.
- Black radish juice will also help. It can be mixed with lavender tincture or essential oil lavender and rub into the sore spot. Then you should wrap yourself in a scarf and lie there for half an hour. During an attack, it is permissible to fumigate the room in which the patient is located. For this you need a wormwood cigar. It is rolled from dry wormwood leaves and set on fire. Fumigation should last no more than 7-10 minutes. Such manipulations must be carried out within a week.
- Heat a glass of buckwheat in a frying pan, pour the cereal into a cotton bag and apply to the sore area. The bag is removed when it has completely cooled down. This procedure is carried out twice a day.
- We treat trigeminal neuralgia with pharmaceutical chamomile - an excellent sedative for NTN. You can make morning tea from it. You should take a certain amount of warm drink into your mouth, but do not swallow it, but hold it for as long as possible.
- Grate the horseradish root on a coarse grater, wrap the resulting pulp in a napkin and apply it as a lotion to the affected area.
- To relieve tension in the body and relieve neuralgic pain, hot baths with the addition of a decoction of young aspen bark are recommended.
Prevention
Of course, influence everything probable reasons the occurrence of the disease is not possible (for example, the congenital narrowness of the canals cannot be changed). However, many factors in the development of this disease can be prevented:
- avoid hypothermia of the face;
- promptly treat diseases that can cause trigeminal neuralgia (diabetes mellitus, atherosclerosis, caries, sinusitis, frontal sinusitis, herpetic infection, tuberculosis, etc.);
- prevention of head injuries.
It should also be taken into account that methods of secondary prevention (i.e. when the disease has already manifested itself once) include high-quality, complete and timely treatment.
So, getting rid of ternary neuralgia is possible. You just need to seek help from specialists in time and undergo an examination. The neurologist will immediately prescribe the necessary medications to combat the disease. If such remedies do not help in the fight against trigeminal neuralgia, they resort to the help of a neurosurgeon who solves the problem surgically.
Trigeminal nerve, n. trigeminus mixed nerve. The motor fibers of the trigeminal nerve arise from it motor nucleus lying in the bridge. The sensory fibers of this nerve approach the pontine nucleus, as well as the nuclei of the midbrain and spinal tract of the trigeminal nerve. This nerve innervates the skin of the face, frontal and temporal regions, the mucous membrane of the nasal cavity and paranasal sinuses, mouth, tongue (2/3), teeth, conjunctiva of the eye, masticatory muscles, muscles of the floor of the mouth (mylohyoid muscle and anterior belly of the biventricular muscles), as well as the muscles that strain the velum palatine and the tympanic membrane. In the area of all three branches of the trigeminal nerve there are vegetative (autonomous) nodes, which were formed from cells that moved out of the rhombencephalon during embryogenesis. These nodes are identical in structure to the intraorgan nodes of the parasympathetic part of the autonomic nervous system.
The trigeminal nerve exits the base of the brain with two roots (sensory and motor) at the point where the pons enters the middle cerebellar peduncle. Sensitive root radix sensoria significantly thicker than the motor root, radix motoria. Next, the nerve goes forward and somewhat laterally, entering into the splitting of the dura mater of the brain - trigeminal cavity,cavum trigemi nale, lying in the area of the trigeminal depression on the anterior surface of the pyramid of the temporal bone. In this cavity there is a thickening of the trigeminal nerve - the trigeminal ganglion, gang lion trigeminale (Gasser knot). The trigeminal ganglion is crescent-shaped and is a cluster of pseudounipolar sensory nerve cells, the central processes of which form a sensory root and go to its sensory nuclei. The peripheral processes of these cells are sent as part of the branches of the trigeminal nerve and end with receptors in the skin, mucous membranes and other organs of the head. The motor root of the trigeminal nerve is adjacent to the trigeminal ganglion from below, and its fibers participate in the formation of the third branch of this nerve.
Three branches of the trigeminal nerve depart from the trigeminal ganglion: 1) the ophthalmic nerve (first branch); 2) maxillary nerve (second branch); 3) mandibular nerve (third branch). The ophthalmic and maxillary nerves are sensory, and the mandibular nerve is mixed, containing sensory and motor fibers. Each of the branches of the trigeminal nerve at its beginning gives off a sensitive branch to the dura mater of the brain.
optic nerve,P.ophthalmicus departs from the trigeminal nerve in the area of its ganglion, is located in the thickness of the lateral wall of the cavernous sinus, and penetrates the orbit through the superior orbital fissure. Before entering the orbit, the optic nerve gives off tentorial (shell) branch, d.tentorii (meningeus). This branch goes posteriorly and branches in the tentorium of the cerebellum. In the orbit, the optic nerve is divided into the lacrimal, frontal and nasociliary nerves (Fig. 173).
1. Lacrimal nerve, P.lacrimdlis runs along the lateral wall of the orbit to the lacrimal gland. Before entering the lacrimal gland, the nerve receives connecting branch, g.communicationscumP.zygomatico connecting it with the zygomatic nerve (nerve of the second branch, P.trigeminus). This branch contains parasympathetic (postganglionic) fibers to innervate the lacrimal gland. The terminal branches of the lacrimal nerve innervate the skin and conjunctiva of the upper eyelid in the region of the lateral canthus. 2. Frontal nerve, P.frontalis goes forward under the upper wall of the orbit, where it divides into two branches. One of its branches is supraorbital nerve, n.supraorbitalis It leaves the orbit through the supraorbital notch and gives off medial and lateral branches, ending in the skin of the forehead. Second branch of the frontal nerve - supratrochlear nerve, n.supratrochledris goes over the block of the superior oblique muscle and ends in the skin of the root of the nose, the lower part of the forehead, in the skin and conjunctiva of the upper eyelid, in the area of the medial corner of the eye. 3. Nasociliary nerve, P.nasocilia ris is directed forward between the medial rectus and superior oblique muscles of the eye and gives off the following branches in the orbit: 1) front And posterior ethmoidal nerves, pp.ethmoiddles an terior et posterior to the mucous membrane of the ethmoid sinuses and to the mucous membrane of the anterior part of the nasal cavity; 2) long ciliary branches, pp.ciliares longi 2-4 branches go forward to the sclera and choroid of the eyeball;
3) subtrochlear nerve, n.infratrochledris passes under the superior oblique muscle of the eye and goes to the skin of the medial corner of the eye and the root of the nose; 4) connecting branch (with ciliary node), d.communications (cum gdnglio cilidri), containing sensory nerve fibers, approaches the ciliary ganglion, which belongs to the parasympathetic part of the autonomic nervous system. Departing from the node 15-20 short ciliary nerves, pp.ciliares breves are directed to the eyeball, providing its sensitive and autonomic innervation.
maxillary nerve,P.maxillaris departs from the trigeminal ganglion, goes forward, exits the cranial cavity through the round foramen into the pterygopalatine fossa.
Even in the cranial cavity, they extend from the maxillary nerve meningeal (middle) branch, d.meningeus (medius), which accompanies the anterior branch of the middle meningeal artery and innervates the dura mater of the brain in the region of the middle cranial fossa. In the pterygopalatine fossa, the infraorbital and zygomatic nerves and nodal branches to the pterygopalatine ganglion depart from the maxillary nerve.
1Infraorbital nerve, P.infraorbitdlis is a direct continuation of the maxillary nerve. Through the inferior orbital fissure, this nerve enters the orbit, passes first in the infraorbital groove and enters the infraorbital canal of the upper jaw. Coming from the canal through the infraorbital foramen to the anterior surface of the upper jaw, the nerve divides into several branches: 1) lower branches of the eyelids,rr. palpebrdles info- riores directed to the skin of the lower eyelid; 2) external nasal branches,rr. nasdles externi branch in the skin of the external nose; 3) superior labial branches,rr. labiates superiores. In addition, on its way, still in the infraorbital groove and in the canal, the infraorbital nerve gives off 4) superior alveolar nerves, n.alveoldres superiores And anterior, middle and posterior alveolar branches,rr. alveoldres superiores anterioresmedius et posteridres which in the thickness of the upper jaw form superior dental plexus,plexus dentdlis superior. Upper dental branchesrr. dentales superiores this plexus innervates the teeth of the upper jaw, and upper gingival branches,rr. gingivdles superiores- gums; 5) internal nasal branches,rr. nasdles interni go to the mucous membrane of the anterior sections of the nasal cavity.
2Zygomatic nerve, P.zygomdticus It arises from the maxillary nerve in the pterygopalatine fossa near the pterygopalatine ganglion and enters the orbit through the inferior orbital fissure. In the orbit, it gives off a connecting branch containing post-nodal parasympathetic fibers from the pterygopalatine ganglion to the lacrimal nerve for secretory innervation of the lacrimal gland. The zygomatic nerve then enters the zygomatic orbital foramen of the zygomatic bone. In the thickness of the bone, the nerve is divided into two branches, one of which is zygomaticotemporal branch, g.zygomaticotempordlis exits through the opening of the same name into the temporal fossa and ends in the skin of the temporal region and the lateral corner of the eye. Another branch - zygomaticofacial, g.zygomaticofacidlis through an opening on the anterior surface of the zygomatic bone it is directed to the skin of the zygomatic and cheek areas.
3 Nodal branches, rr. gangliondres , containing sensory fibers, go from the maxillary nerve (in the pterygopalatine fossa) to the pterygopalatine ganglion and to the branches extending from it.
Pterygopalatine ganglion, ganglion pterygopalatinum refers to the parasympathetic part of the autonomic nervous system. This unit is suitable for: 1) nodal branches (sensitive- from the maxillary nerve), the fibers of which pass through the node in transit and are part of the branches of this node; 2) preganglionic parasympathetic fibers from the nerve of the pterygoid canal, which end in the pterygopalatine ganglion on the cells of the second neuron. The processes of these cells emerge from the node as part of its branches; 3) postganglionic sympathetic fibers from the nerve of the pterygoid canal, which pass through the node in transit and are part of the branches emerging from this node. Branches of the pterygopalatine ganglion:
1medial and lateral superior posterior nasal branches,rr. nasdles posteriores superiores middles et laterdles penetrate through the sphenopalatine foramen and innervate the mucous membrane of the nasal cavity, including its glands. The largest of the superior medial branches is nasopalatine nerve, n.nasopala- tinus (nasopalatini), lies on the nasal septum, then is directed through the incisive canal to the mucous membrane of the hard palate;
2greater and lesser palatine nerves, pL palatinus major et tin. palatini minores through the channels of the same name they follow to the mucous membrane of the hard and soft palate;
3inferior posterior nasal branches,rr. nasdles posteriores in- feriores are branches of the greater palatine nerve, pass through the palatine canal and innervate the mucous membrane of the lower parts of the nasal cavity.
mandibular nerve,P.mandibuldris exits the cranial cavity through the foramen ovale. It contains motor and sensory nerve fibers. When leaving the foramen ovale, motor branches depart from the mandibular nerve to the chewing muscles of the same name.
Motor branches: 1) masticatory nerve, n.mas- setericus; 2) deep temporal nerves, pp.tempordles profundi; 3) lateral and medial pterygoid nerves, pp.pterygoidei laterlis et medlis (Fig. 175); 4) nerve of the muscle that tenses the velum palatine, n.muscles tensoris veil palatini; 5) nerve of the tensor tympani muscle, n.muscles tensoris tympani.
Sensitive branches:
1Meningeal branch, G.meningeus returns to the cranial cavity through the foramen spinosum (accompanies the middle meningeal artery) for innervation of the dura mater of the brain in the region of the middle cranial fossa;
2Buccal nerve, ". buccdlis first it goes between the heads of the lateral pterygoid muscle, then comes out from under the anterior edge of the masticatory muscle, lies on the outer surface of the buccal muscle, pierces it and ends in the mucous membrane of the cheek, as well as in the skin of the corner of the mouth.
3Auriculotemporal nerve, P.auriculotempordlis begins with two roots that cover the middle meningeal artery, and then unite into one trunk. Having passed along the inner surface of the coronoid process of the mandible, the nerve bypasses its neck from behind and rises anteriorly from the cartilage of the external auditory canal, accompanying the superficial temporal artery. They arise from the auriculotemporal nerve anterior auricular nerves, pp.auriculars anteriores to the front of the ear; nerves of the external auditory canal, n.medtus acustici externi; branches of the eardrum,rr. Membrdnae tympani to the eardrum; superficial temporal branches,rr. tempordles super fiddles to the skin of the temporal region; parotid branches,rr. parotidei containing postnodal parasympathetic secretory nerve fibers to the parotid salivary gland. These fibers joined the auriculotemporal nerve as part of connecting branch (with the auriculotemporal nerve), d.communications (cum n. auriculotempordlis).
Our nervous system is usually divided into several sections. They distinguish, and everyone knows this from the school curriculum, into a central and a peripheral department. The autonomic nervous system is distinguished separately. The central section is nothing more than the spinal cord and brain. The peripheral part, directly connected to the central nervous system (CNS), is represented by the spinal and cranial nerves. Through them, the central nervous system transmits various kinds of “information” from receptors located in different parts of our body.
General idea of the structure of cranial nerves
Location of cranial nerves, ventral view
In total there are 12 of them or sometimes 13. Why sometimes thirteen? The fact is that only some of the authors call one of them, the intermediate one, the 13th pair.
More about the trigeminal nerve
The fifth, one of the largest, pair of cranial nerves, namely (trigeminal nerve - nervus trigeminus). Let us dwell in more detail on the anatomy and diagram of the trigeminal nerve. Its fibers originate in the nuclei of the brain stem. In this case, the nuclei are located in the projection of the bottom of the fourth ventricle. To more accurately understand where the trigeminal nerve is located in humans, see the photo.
Exit point and location of the main branches of the trigeminal nerve
General structure
The nervus trigeminus itself is mixed, that is, it carries motor (motor) and sensitive (sensory) fibers. Motor fibers transmit information from muscle cells (myocytes), and sensory fibers “serve” various receptors. The trigeminal facial nerve exits the brain just in the area where the pons and middle cerebellar peduncle converge. And it immediately “forks out.”
Main branches
Imagine a tree branch from which thinner branches diverge in different directions. Introduced? The same goes for the trigeminal nerve. In the anatomy of the trigeminal nerve, its branches also diverge to the sides with many branches. There are three branches in total:
main branches of the trigeminal nerve and areas of their innervation
Ophthalmic branch
The ophthalmic (Latin name is nervus ophtalmicus) is the first (1) branch of the trigeminal nerve (in the photo the uppermost). Entirely composed of sensory fibers. This means that it only transmits data from different receptors. For example, receptors for tactile, temperature, pain sensitivity. If we continue the analogy with the tree, the optic nerve also branches, only this happens in the orbit. Thus, the superior orbital fissure (n.ophthalmicus enters the orbit through it) is one of the points of exit of the trigeminal nerve from the cranial cavity. Surprisingly, n.ophthalmicus also branches into several branches:
- the frontal is the longest.
- the lacrimal gland, which passes between the muscles responsible for eye movements and innervates the lacrimal gland.
- nasociliary, it is she who innervates our eyelashes and part of the nasal epithelium.
Maxillary branch
Maxillary (Latin name - nervus maxillaris) - second (2) branch. Sensory, that is, it also consists of one hundred percent sensory fibers. It branches in the orbit, however, it gets there not through the upper, but through the lower orbital fissure (it becomes the second exit point from the cranial cavity, where the ternary nerve is located along with the nuclei). Let's look at the branches of the maxillary nerve. An important part, which is a network of fibers extending from n. maxillaris is the upper dental plexus, as the name implies, its function is to provide communication between the central nervous system and receptors located in the gums and teeth. As soon as the maxillary nerve passes into the infraorbital groove, it becomes infraorbital. The zone of its innervation becomes clear from the names of its small branches: external nasal, upper labial, lower branches of the eyelids. The zygomatic nerve is the only branch of the maxillary nerve that separates from the latter outside the orbit. But then it still penetrates into the orbit, however, not through the lower, but through the upper orbital fissure. And it innervates mainly the skin of the face, in the area adjacent to the cheekbones, as the name implies.
Mandibular branch
The mandibular (Latin name is nervus mandibularis) is the third (3) branch of the trigeminal nerve. The sensory-motor branch, unlike the two previous branches, is mixed and contains sensory and motor fibers. She is the largest. It exits the skull near the foramen magnum, through the foramen ovale. Upon exiting, it almost immediately branches into several branches.
Sensory (sensory) branches of the mandibular nerve:
- Lower alveolar (Latin name - nervus alveolaric inferior) - remember just above we talked about the upper dental plexus? So, there is also a lower one, it is formed precisely from the fibers of this branch of the n.mandibularis. That's right, because the lower teeth and gums cannot remain without innervation, right?
- Buccal (Latin name n. buccalis) - passes through the buccal muscle and approaches the epithelium of the cheek.
- Lingual (Latin name - nervus lingualis) - its “coverage area” becomes, as the name suggests, the mucous membrane of the tongue, and not all of it, but only 60 - 70% located towards the front.
- The meningeal branch (Latin name ramus meningeus) - makes a 180-degree turn and approaches the dura mater, and for this it returns to the cranial cavity.
- Auricular-temporal (Latin name nervus auriculotemporalis) - carries information from the ear and the “adjacent territory”, the auricle along with the ear canal, the skin in the temple area
Motor fibers of the n.mandibularis (mandibular nerve):
- The chewing branch is needed so that the chewing muscles contract in time when we see some tasty food.
- The deep temporal branches - in general, are needed for the same thing, only they innervate slightly different masticatory muscles.
- The pterygoid branches (there are two of them, lateral and medial) also innervate several other muscles needed for chewing.
The largest nerve related to the cranial brain is the trigeminal nerve, which, as the name implies, contains three main branches and many smaller ones. It is responsible for the mobility of the facial muscles, provides the ability to make chewing movements and bite off food, and also gives sensitivity to the organs and skin of the anterior head area.
In this article we will understand what the trigeminal nerve is.
Layout diagram
The branched trigeminal nerve, which has many branches, originates in the cerebellum, comes from a pair of roots - motor and sensory, and envelops all the facial muscles and some parts of the brain in a web of nerve fibers. Close connection with spinal cord allows you to control various reflexes, even those associated with the respiratory process, such as yawning, sneezing, blinking.
The anatomy of the trigeminal nerve is as follows: from the main branch, approximately at the level of the temple, thinner ones begin to separate, in turn, branching and thinning further and lower. The point at which separation occurs is called the Gasser, or trigeminal, node. The processes of the trigeminal nerve pass through everything on the face: eyes, temples, mucous membranes of the mouth and nose, tongue, teeth and gums. Thanks to impulses sent by nerve endings to the brain, feedback occurs that provides sensory sensations.
This is where the trigeminal nerve is located.
The finest nerve fibers, literally penetrating all parts of the facial and parietal zones, allow a person to feel touch, experience pleasant or discomfort, move the jaws, eyeballs, lips, express various emotions. Intelligent nature has endowed the nervous network with exactly that amount of sensitivity that is necessary for a calm existence.
Main branches
The anatomy of the trigeminal nerve is unique. The trigeminal nerve has only three branches; from them there is further division into fibers leading to organs and skin. Let's look at them in more detail.
1 branch of the trigeminal nerve is the optic or orbital nerve, which is only sensory, that is, transmitting sensations, but not responsible for the work of motor muscles. With its help, information is exchanged between the central nervous system and nerve cells of the eyes and orbits, sinuses and mucous membrane of the frontal sinus, forehead muscles, lacrimal gland, and meninges.
Three more thinner nerves branch off from the optic nerve:
- tearful;
- frontal;
- nasociliary.
Since the parts that make up the eye must move, and the orbital nerve cannot provide this, a special autonomic node called the ciliary node is located next to it. Thanks to the connecting nerve fibers and the additional nucleus, it provokes contraction and straightening of the pupillary muscles.
Second branch
The trigeminal nerve on the face also has a second branch. The maxillary, zygomatic or infraorbital nerve is the second major branch of the trigeminal and is also intended to transmit only sensory information. Through it, sensations go to the wings of the nose, cheeks, cheekbones, upper lip, gums and dental nerve cells of the upper row.
Accordingly, from this thick nerve comes a large number of medium and thin branches passing through different parts of the face and mucous tissues and combined for convenience into the following groups:
- maxillary main;
- zygomatic;
- cranial;
- nasal;
- facial;
- infraorbital.
Here, too, there is a parasympathetic vegetative ganglion, called the pterygopalatine ganglion, which promotes salivation and mucus secretion through the nose and maxillary sinuses.
Third branch
The 3rd branch of the trigeminal nerve is called the mandibular nerve, which performs both providing sensitivity to certain organs and areas, and the function of moving the muscles of the oral cavity. It is this nerve that is responsible for the ability to bite off, chew and swallow food, and encourages the movement of the muscles necessary for speaking and located in all the parts that make up the mouth area.
The following branches of the mandibular nerve are distinguished:
- buccal;
- lingual;
- alveolar lower - the largest, giving off a number of thin nerve processes that form the lower dental ganglion;
- auriculotemporal;
- chewing;
- lateral and medial pterygoid nerves;
- maxillohyoid.
The mandibular nerve has the most parasympathetic formations that provide motor impulses:
- ear;
- submandibular;
- sublingual.
This branch of the trigeminal nerve transmits sensitivity to the lower row of teeth and the lower gum, lip and jaw as a whole. The cheeks also receive sensations partly with the help of this nerve. The motor function is performed by the masticatory, pterygoid and temporal branches.
These are the main branches and exit points of the trigeminal nerve.
Causes of defeat
Inflammatory processes of various etiologies affecting the tissues of the trigeminal nerve lead to the development of a disease called neuralgia. Based on its location, it is also called “facial neuralgia.” It is characterized by a sudden paroxysm of sharp pain piercing different parts of the face.
This is how the trigeminal nerve is damaged.
The causes of this pathology are not fully understood, but many factors are known that can provoke the development of neuralgia.
The trigeminal nerve or its branches are compressed under the influence of the following diseases:
- cerebral aneurysm;
- atherosclerosis;
- stroke;
- osteochondrosis, causing increased intracranial pressure;
- congenital defects of blood vessels and skull bones;
- neoplasms that arise in the brain or on the face where the branches of the nerve pass;
- injury and scarring of the face or jaw joints, temples;
- formation of adhesions caused by infection.
Diseases of viral and bacterial nature
- Herpes.
- HIV infection
- Polio.
- Chronic otitis media, mumps.
- Sinusitis.
Diseases affecting the nervous system
- Meningitis of various origins.
- Epilepsy.
- Cerebral palsy.
- Encephalopathy, cerebral hypoxia, leading to a lack of supply of substances necessary for full functioning.
- Multiple sclerosis.
Surgery
The trigeminal nerve on the face can be damaged as a result of surgery in the area of the face and oral cavity:
- damage to jaws and teeth;
- consequences of incorrect anesthesia;
- incorrectly performed dental procedures.
The anatomy of the trigeminal nerve is truly unique and therefore this area is very vulnerable.
Characteristics of the disease
The pain syndrome can be felt only on one side or affect the entire face (much less often), and can affect only the central or peripheral parts. In this case, the features often become asymmetrical. Attacks of varying strength last a maximum of a few minutes, but can cause extremely unpleasant sensations.
This is how much discomfort the trigeminal nerve can cause. A diagram of possible affected areas is shown below.
The process can cover different parts of the trigeminal nerve - branches individually or some together, the nerve sheath or its entirety. Most often women aged 30-40 years are affected. Paroxysms of pain in severe neuralgia can be repeated many times throughout the day. Patients experiencing this disease describe the attacks as being like electric shocks, and the pain can be so severe that the person temporarily becomes blind and ceases to perceive the world around him.
Facial muscles can become so sensitive that any touch or movement provokes a new attack. Appear nervous tics, spontaneous contractions of the facial muscles, mild convulsions, discharge of saliva, tears or mucus from the nasal passages. Constant attacks significantly complicate the lives of patients; some try to stop talking and even eating, so as not to further affect the nerve endings.
Quite often, facial paresthesia is observed for a certain time before the paroxysm. This feeling is reminiscent of pain in a sedentary leg - goosebumps, tingling and numbness of the skin.
Possible complications
Patients who delay seeing a doctor run the risk of developing many problems in a few years:
- weakness or atrophy of the masticatory muscles, most often from trigger zones (areas whose irritation causes painful attacks);
- asymmetry of the face and a raised corner of the mouth, reminiscent of a grin;
- skin problems – peeling, wrinkles, dystrophy;
- loss of teeth, hair, eyelashes, early gray hair.
Diagnostic methods
First of all, the doctor collects a complete medical history, finding out what diseases the patient had to endure. Many of them can provoke the development of trigeminal neuralgia. Then the course of the disease is recorded, the date of the first attack and its duration are noted, and associated factors are carefully checked.
It is necessary to clarify whether paroxysms have a certain periodicity or occur, at first glance, chaotically, and whether there are periods of remission. Next, the patient shows the trigger zones and explains what influences and what force must be applied to provoke an exacerbation. The anatomy of the trigeminal nerve is also taken into account here.
The location of the pain is important - one or both sides of the face are affected by neuralgia, as well as whether painkillers, anti-inflammatory and antispasmodic drugs help during an attack. Additionally, the symptoms that can be described by the patient observing the picture of the disease are clarified.
The examination will need to be carried out both during a quiet period and during the onset of an attack - this way the doctor will be able to more accurately determine the state of the trigeminal nerve, which parts of it are affected, give a preliminary conclusion about the stage of the disease and a prognosis for the success of treatment.
How is the trigeminal nerve diagnosed?
Important Factors
Typically, the following factors are assessed:
- The patient's state of mind.
- Appearance of the skin.
- The presence of cardiovascular, neurological, digestive disorders and pathology of the respiratory system.
- The ability to touch trigger areas on the patient’s face.
- The mechanism of occurrence and spread of pain syndrome.
- The patient's behavior is numbness or active actions, attempts to massage the nerve area and the painful area, inadequate perception of surrounding people, absence or difficulties with verbal contact.
- The forehead becomes covered with sweat, the pain area turns red, there is strong discharge from the eyes and nose, and swallowing of saliva.
- Facial muscle spasms or tics.
- Changes in breathing rhythm, pulse, blood pressure.
This is how the trigeminal nerve is examined.
An attack can be temporarily stopped by pressing on certain nerve points or blocking these points with novocaine injections.
Magnetic resonance and computed tomography, electroneurogathia and electroneuromyography, as well as an electroencephalogram are used as certification methods. Additionally, a consultation with an ENT specialist, neurosurgeon and dentist is usually prescribed to identify and treat diseases that can provoke the appearance of facial neuralgia.
Treatment
Complex therapy is always aimed primarily at eliminating the causes of the disease, as well as relieving symptoms that cause pain. Typically, the following drugs are used:
- Anticonvulsants: “Finlepsin”, “Difenin”, “Lamotrigine”, “Gabantine”, “Stazepin”.
- Muscle relaxants: “Baklosan”, “Lioresal”, “Mydocalm”.
- Vitamin complexes containing group B and omega-3 fatty acids.
- Antihistamines, mainly Diphenhydramine and Pipalfen.
- Medicines that have a sedative and antidepressant effect: Glycine, Aminazine, Amitriptyline.
In case of severe lesions of the trigeminal nerve, it is necessary to use surgical interventions aimed at:
- to alleviate or eliminate diseases that provoke attacks of neuralgia;
- decreased sensitivity of the trigeminal nerve, a decrease in its ability to transmit information to the brain and central nervous system;
The following types of physiotherapy are used as additional methods:
- irradiation of the neck and face area with ultraviolet radiation;
- exposure to laser irradiation;
- treatment using ultra-high frequencies;
- electrophoresis with drugs;
- Bernard diadynamic current;
- manual therapy;
- acupuncture.
All treatment methods, medications, course and duration are prescribed exclusively by the doctor and are selected individually for each patient, taking into account his characteristics and the picture of the disease.
We looked at where the trigeminal nerve is located, as well as the causes of its damage and treatment methods.
Most of them are cranial, that is, they come from the brain. one such nerve is the trigeminal nerve. What is the anatomy of the trigeminal nerve?
What is it?
The trigeminal nerve is a mixed type nerve in its structure. Belongs to the 5th pair of cranial nerves.
It includes sensory (afferent, centripetal) and motor (centrifugal) fibers, due to which impulses from both superficial (pain and temperature) and deep (proprioceptive) receptors are transmitted along this nerve. Motor innervation is carried out by the motor nucleus, which innervates mainly the masticatory muscles. What is the anatomy of the trigeminal nerve and the localization of its branches?
The nerve exits the brain in the pons area. Coming out of the brain, most of it passes through the pyramid. At its top, the nerve is divided into three branches: orbital (r.ophthalmicus), maxillary (r.maxillaris) and mandibular (r.mandibularis).
This nerve is of interest to neurologists as it innervates the entire facial area. Its lesions are quite often observed due to hypothermia, injuries to the facial area, and certain diseases of the musculoskeletal system.
What is the anatomy of the trigeminal nerve and its branches?
Orbital nerve

The first branch of the trigeminal nerve is the orbital nerve or nervus ophthalmicus.
This is the thinnest branch arising from the trigeminal nerve. It primarily performs the function of reception. Innervates the skin of the forehead, some parts of the temporal and parietal region, the upper eyelid, the back of the nose, some sinuses of the facial bones and partially the mucous membrane of the nasal cavity.
The nerve includes about thirty relatively small bundles. The nerve enters the orbit at the outer wall of the ophthalmic sinus, where it gives off branches to the trochlear sinus and in the area of the superior orbital notch, the nerve is divided into three smaller and thinner bundles - the lacrimal, frontal and ciliary nerves.
Their close localization to the eyeball often leads to their damage as a result of injuries to the orbit or supraorbital region.
The ciliary nerve, in turn, forms the ciliary ganglion, located on the border of the inner and middle third. It includes parasympathetic nerve endings involved in the innervation of the glands of the eye and the periorbital region.
Maxillary nerve
Another branch of the trigeminal nerve is the maxillary or nervus maxillaris.
It exits the cranial cavity through the oval window. From there it enters the pterygopalatine fossa. Passing through it, the nerve continues into the infraorbital, passing through the inferior orbital foramen. Having passed through it, the nerve passes through the canal of the same name on the lower wall of the orbit. It enters the face through the inferior orbital foramen, where it splits into smaller branches. They form connections with branches and innervate the skin of the lower eyelid, upper lip and lateral surface of the face. In addition, branches such as the zygomatic nerve, the superior alveolar branches that form a plexus near the teeth, and the ganglion branches that connect the maxillary nerve with the pterygopalatine ganglion depart from the maxillary nerve.
Damage to this nerve is observed in cases of massive facial injuries, neuritis, and operations on the teeth and sinuses.
Mandibular nerve
The third and most complex branch of the trigeminal nerve is the mandibular or nervus mandibularis. In its composition, in addition to the sensory branches, it contains almost the entire part of the motor root of the trigeminal nerve, emerging from the motor nucleus, nucleus motorius, to the muscles of the lower jaw. As a result of this arrangement, it innervates these muscles, as well as the skin that covers them. The nerve leaves the skull through the foramen ovale (oval window or opening), after which it divides into 2 groups of branches:
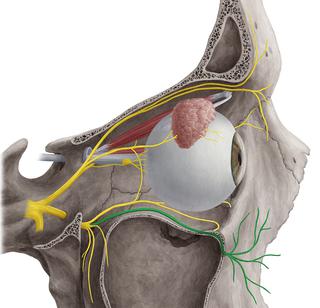
We can assume that it is this branch that continues the trigeminal nerve. The anatomy, diagram of this nerve (structure) and its properties (mixed nerve fiber) allow us to consider this branch to be terminal. Despite the fact that it forms the inferior alveolar nerve plexus, its ending point can be considered the entrance to the mandibular canal.
Course of nerve fibers
What is the anatomy of the trigeminal nerve (the structure and course of its branches)?
The structure of the trigeminal nerve is similar to that of any of the spinal nerves; it has a special large node - the trigeminal ganglion. This formation is located in the middle cranial fossa. It is surrounded on all sides by layers of the dura mater. The node has dendrites that form three large main branches of the trigeminal nerve. The sensitive nerve root penetrates through the middle cerebellar peduncles, where it closes on three nuclei of the brain - superior and middle, each of which contains specific sensory neurons. The motor part of the nerve begins from the motor nucleus - nucleus motorius.

Due to this location, the nerve can be exposed to influence from both the brain and surrounding tissues, which is why it is of particular interest to neurologists.
What are the main types of lesions characteristic of the nerve?
Trigeminal nerve diseases
What processes influence the functional ability of this formation, and how can the trigeminal nerve be affected?
The anatomy of its course predisposes to the development of channelopathies - infringement of the branches of the nerve passing through the canal or opening by surrounding formations. In this case, knowledge of the topography of the nerve and some topical signs allows us to determine the level of its damage and take appropriate measures.
Another equally important factor is the influence of surrounding tissues. Most often, nerves are affected by brain tumors. As they grow, they contribute to its compression and the appearance of the corresponding clinical picture.
The anatomy of the trigeminal nerve (knowledge of its branches and the places of its projection onto the face) allows you to determine the exit points of the nerve branches and stimulate them using electrophysiological methods, or, taking into account the location of the branches, carry out appropriate treatment of the underlying disease that led to the appearance of pathological symptoms.
Trigeminal nerve examination
The study of the function of the trigeminal nerve is carried out to determine the sensitivity of the areas of the skin that it innervates, as well as the patient’s ability to tense and relax the masticatory muscles. The nerve is examined by palpating its exit points on the face. How to determine how sensitive the trigeminal nerve is? Its anatomy allows us to determine the activity of sensory neurons located under the skin.

Sensitivity determination is carried out with cotton wool or a swab soaked in a cold or hot solution. Pain sensitivity is tested by touching the needle.
For check motor function ask the patient to perform several chewing movements.
In the presence of pathology, a change in sensitivity is observed in one or more zones of innervation, or the patient is unable to perform chewing movements correctly. There is a deviation of the jaw to the painful side or excessive muscle spasm. Tension in the masticatory muscles is determined by pressing them during the act of chewing.
Why do you need to know topography?
Topographic anatomy of the trigeminal nerve is necessary for precise definition affected area. Knowing where each branch goes, what clinical signs are characteristic of its damage and how they can be complicated, you can decide on the scope and treatment plan.

Knowledge of the location and course of the branches of this nerve rests with neurologists and neurosurgeons. It is these specialists who, for the most part, encounter diseases in which the trigeminal nerve is affected. Anatomy (photo obtained using MRI) allows you to determine treatment tactics and take appropriate measures.
When the first signs of damage to one or another branch of the nerve appear, you must immediately seek help from a doctor of appropriate specialization to determine the diagnosis and draw up a treatment algorithm.

