Similar documents
Identification of teeth based on crown curvature, crown angle and root deviation. Anatomical characteristics of a tooth, allowing one to determine its group affiliation. Anatomy of incisors, canines, premolars, molars. Closing of the teeth of the upper and lower jaws.
presentation, added 12/17/2013
The main sections that make up the human oral cavity. Innervation - trigeminal and facial nerve. Sectional structure of a tooth. Key functions of teeth. The tongue is an entirely muscular organ. Muscles that provide movement of the tongue and its individual parts.
presentation, added 04/23/2014
Periods of dental development in children. Morphological features of the intrauterine period. The time from birth to the beginning of the eruption of baby teeth, the period of formation of their bite. Formed primary and secondary dentitions. Period of occlusion of permanent teeth.
presentation, added 12/16/2015
Development salivary glands and teeth. Motor function primary department digestive tract. The structure and wall of the esophagus. The structure of the wall of the digestive tract: mucous membrane, muscular layer and submucosal layer. The structure of the large intestine and its wall.
abstract, added 03/25/2009
general characteristics female genital organs, structure and functions of the uterus and its appendages. Features of the mucous and muscular membranes. The relationship of the uterus to the peritoneum and its ligamentous apparatus. Blood flow, lymph flow and innervation of the organ. Structure and functions of the ovaries.
abstract, added 09/04/2011
Study of the structure of tooth tissues, structural features of enamel prisms, the main structural and functional units of enamel. An overview of the composition of dentin, the tissue that forms the bulk of the tooth and determines its shape. Analysis of the process of formation of cellular cement.
presentation, added 02/07/2012
Teeth: milk teeth, permanent teeth, their formula and structure. Stomach: position, parts, wall structure, functions. Structural and functional units of the lungs, liver, kidneys. Heart: size, shape, position, borders. Features of structure and functions nervous system.
course of lectures, added 06/04/2012
The functions of teeth, their active participation in the basic vital functions of the body: nutrition, breathing and the formation of sounds. Rules for dental care, cleaning, hygiene and preventive measures aimed at maintaining oral health.
presentation, added 05/28/2010
Regulation of activities internal organs through hormones. Structure, functions, blood supply, lymphatic drainage and innervation of the pituitary gland, vessels and nerves, pineal gland, thyroid gland, parathyroid gland, pancreas, adrenal glands, thymus.
presentation, added 04/27/2016
Classification of tissues, types of epithelial tissues, their structure and functions. Supportive, trophic and protective function of connective tissues. Functions of nervous and muscle tissues. The concept of organs and organ systems, their individual, gender, age differences.
The speech apparatus is a set of interacting human organs that actively participate in the production of sounds and speech breathing, thereby forming speech. The speech apparatus includes the organs of hearing, articulation, breathing, and Today we will take a closer look at the structure of the speech apparatus and the nature of human speech.
Production of sounds
Today, the structure of the speech apparatus can safely be considered 100% studied. Thanks to this, we have the opportunity to find out how sound is born and what causes speech disorders.
Sounds are generated due to the contraction of muscle tissue of the peripheral speech apparatus. When starting a conversation, a person automatically inhales air. From the lungs, air flows into the larynx, nerve impulses cause vibration, and these, in turn, create sounds. Sounds form words. Words - into sentences. And suggestions - into intimate conversations.
The speech apparatus, or, as it is also called, the voice apparatus, has two sections: central and peripheral (executive). The first consists of the brain and its cortex, subcortical nodes, pathways, brainstem nuclei and nerves. The peripheral one, in turn, is represented by a set of executive organs of speech. It includes: bones, muscles, ligaments, cartilage and nerves. Thanks to the nerves, the listed organs receive tasks.
Central department
Like other manifestations of the nervous system, speech occurs through reflexes, which, in turn, are connected to the brain. The most important departments The brain responsible for speech reproduction is the frontal parietal and occipital regions. For right-handed people this role is played by right hemisphere, and for left-handers - left.
The frontal (inferior) gyri are responsible for the production of spoken language. The convolutions located in the temporal zone perceive all sound stimuli, that is, they are responsible for hearing. The process of understanding heard sounds occurs in the parietal region of the cerebral cortex. well and occipital part responsible for the function of visual perception writing. If we take a closer look at the child’s speech apparatus, we will notice that his occipital part is especially actively developing. Thanks to it, the child visually records the articulation of his elders, which leads to the development of his oral speech.
The brain interacts with the peripheral region through centripetal and centrifugal pathways. The latter send brain signals to the organs of the speech apparatus. Well, the first ones are responsible for delivering the response signal.

The peripheral speech apparatus consists of three more sections. Let's look at each of them.
Respiratory section
We all know that breathing is the most important physiological process. A person breathes reflexively, without thinking about it. The breathing process is regulated by special centers of the nervous system. It consists of three stages, continuously following each other: inhalation, short pause, exhalation.
Speech is always formed on the exhale. Therefore, the air flow created by a person during a conversation performs articulatory and voice-forming functions simultaneously. If this principle is violated in any way, speech is immediately distorted. This is why many speakers pay attention to speech breathing.
The respiratory organs of the speech apparatus are represented by the lungs, bronchi, intercostal muscles and diaphragm. The diaphragm is an elastic muscle that, when relaxed, has a dome shape. When it contracts together with the intercostal muscles, rib cage increases in volume and inhalation occurs. Accordingly, when you relax, exhale.
Voice department
We continue to consider the sections of the speech apparatus. So, the voice has three main characteristics: strength, timbre and height. Vibration of the vocal cords causes the flow of air from the lungs to become vibrations of small air particles. These pulsations, transmitted to environment, create the sound of a voice.

Timbre can be called sound coloring. It is different for all people and depends on the shape of the vibrator that creates vibrations of the ligaments.
Articulation department
The speech articulatory apparatus is simply called sound-pronouncing. It includes two groups of organs: active and passive.
Active organs
As the name suggests, these organs can be mobile and are directly involved in the formation of the voice. They are represented by the tongue, lips, soft palate and lower jaw. Since these organs are made up of muscle fibers, they can be trained.
When the speech organs change their position, in various parts constrictions and closures appear in the sound-producing apparatus. This leads to the formation of a sound of one or another nature.
A person's soft palate and lower jaw can move up and down. With this movement they open or close the passage into the nasal cavity. The lower jaw is responsible for the formation of stressed vowels, namely the sounds: “A”, “O”, “U”, “I”, “Y”, “E”.
The main organ of articulation is the tongue. Thanks to the abundance of muscles, he is extremely mobile. The tongue can: shorten and lengthen, become narrower and wider, be flat and curved.
Human lips, being a mobile formation, take an active part in the formation of words and sounds. The lips change their shape and size to enable the pronunciation of vowel sounds.
The soft palate, or, as it is also called, the velum palatine, is a continuation of the hard palate and lies at the top oral cavity. It, like the lower jaw, can move down and up, separating the pharynx from the nasopharynx. The soft palate originates behind the alveoli, near the upper teeth and ends with a small tongue. When a person pronounces any sounds other than “M” and “N”, the velum of the palate rises. If for some reason it is lowered or motionless, the sound comes out “nasal”. The voice comes out nasal. The reason for this is simple - when the velum is lowered, sound waves together with the air they enter the nasopharynx.

Passive organs
The human speech apparatus, or rather its articulatory section, also includes fixed organs that support the moving ones. These are teeth nasal cavity, hard palate, alveoli, larynx and pharynx. Despite the fact that these organs are passive, they provide a huge impact on
Now that we know what the human vocal apparatus consists of and how it works, let's consider the main problems that may affect it. Problems with the pronunciation of words, as a rule, arise from the immaturity of the speech apparatus. When certain parts of the articulation department become ill, this affects the correct resonance and clarity of sound pronunciation. Therefore, it is important that the organs that are involved in the formation of speech are healthy and work in full harmony.
The speech apparatus may be impaired by various reasons, since this is a rather complex mechanism of our body. However, among them there are problems that occur most often:
- Defects in the structure of organs and tissues.
- Incorrect use of the speech apparatus.
- Disorders of the corresponding parts of the central nervous system.
If you have problems with speech, do not put them off long box. And the reason here is not only that speech is the most important factor in the formation of human relationships. Typically, people who have impaired speech apparatus not only speak poorly, but also experience difficulties in breathing, chewing food and other processes. Therefore, by eliminating the lack of speech, you can get rid of a number of problems.

Preparing the speech organs for work
In order for your speech to be beautiful and relaxed, you need to take care of it. This usually takes place in preparation for public speaking, when any stumble and mistake can cost your reputation. The speech organs are prepared for work in order to activate (adjust) the main muscle fibers. Namely, the muscles that are involved in speech breathing, the resonators that are responsible for the sonority of the voice, and the active organs that are responsible for the intelligible pronunciation of sounds.
The first thing to remember is that a person’s speech apparatus functions better with correct posture. This is a simple but important principle. To make your speech clearer, you need to keep your head straight and your back straight. The shoulders should be relaxed and the shoulder blades should be slightly squeezed. Now nothing stops you from saying beautiful words. By getting used to correct posture, you can not only take care of clear speech, but also gain a more advantageous appearance.
For those who speak a lot due to their occupation, it is important to learn to relax the organs responsible for the quality of speech and restore their full functionality. Relaxation of the speech apparatus is ensured by performing special exercises. It is recommended to do them immediately after a long conversation, when the vocal organs are very tired.
Relaxation pose
You may have already come across such concepts as posture and relaxation mask. These two exercises are aimed at relaxing the muscles or, as they also say, removing the muscles. In fact, they are not anything complicated. So, to take a relaxation pose, you need to sit on a chair and bend slightly forward, bowing your head. In this case, the legs should stand with their entire feet and form a right angle with each other. They should also bend at right angles. This can be achieved by selecting a suitable chair. The arms hang down, resting the forearms lightly on the hips. Now you need to close your eyes and relax as much as possible.

To ensure that rest and relaxation are as complete as possible, you can engage in some forms of auto-training. At first glance, it seems that this is the pose of a dejected person, but in fact it is quite effective for relaxing the entire body, including the speech apparatus.
Relaxation mask
This simple technique is also very important for speakers and those who, due to the specific nature of their work, talk a lot. There is nothing complicated here either. The essence of the exercise is to alternately tense various facial muscles. You need to “put on” different “masks”: joy, surprise, melancholy, anger, and so on. Having done all this, you need to relax your muscles. It's not difficult to do this at all. Simply make the sound “T” as you exhale gently and leave your jaw in a loose, lowered position.

Relaxation is one of the elements of hygiene of the speech apparatus. In addition to this, this concept includes protection from colds and hypothermia, avoiding irritants of the mucous membrane and training speech.
Conclusion
This is how interesting and complex our speech apparatus is. In order to fully enjoy one of the most important human gifts - the ability to communicate, you need to monitor the hygiene of the vocal apparatus and treat it with care.
 An organ (from the gr. organon - tool, instrument, organ) is a phylogenetically formed complex of various tissues, united by development, general structure and function. An organ is an integral formation that has a certain form, structure, function, development and position in the body that is unique to it.
An organ (from the gr. organon - tool, instrument, organ) is a phylogenetically formed complex of various tissues, united by development, general structure and function. An organ is an integral formation that has a certain form, structure, function, development and position in the body that is unique to it.
 System (from the gr. systema - a whole made up of parts; connection) - a collection of organs that are similar in their general structure, functions, origin and development. The dentitions form a single functional system- dentofacial, the unity and stability of which is ensured by the alveolar process of the upper and alveolar parts of the lower jaw, periodontium.
System (from the gr. systema - a whole made up of parts; connection) - a collection of organs that are similar in their general structure, functions, origin and development. The dentitions form a single functional system- dentofacial, the unity and stability of which is ensured by the alveolar process of the upper and alveolar parts of the lower jaw, periodontium.
 Apparatus (from Latin apparatus) is a union of systems and individual organs that function in a similar direction or have a common origin and location.
Apparatus (from Latin apparatus) is a union of systems and individual organs that function in a similar direction or have a common origin and location.
 The chewing vocal apparatus is a complex of interconnected and interacting systems and individual organs involved in chewing, breathing, sound production and speech.
The chewing vocal apparatus is a complex of interconnected and interacting systems and individual organs involved in chewing, breathing, sound production and speech.
 The masticatory speech apparatus includes: – facial skeleton and temporomandibular joints; – chewing muscles; – organs designed for grasping, moving food, forming a bolus of food, for swallowing, as well as the sound radicular system: lips, cheeks with their facial muscles, palate, tongue; – organs for biting, crushing and grinding food (teeth), and its enzymatic processing (salivary glands).
The masticatory speech apparatus includes: – facial skeleton and temporomandibular joints; – chewing muscles; – organs designed for grasping, moving food, forming a bolus of food, for swallowing, as well as the sound radicular system: lips, cheeks with their facial muscles, palate, tongue; – organs for biting, crushing and grinding food (teeth), and its enzymatic processing (salivary glands).
 The upper jaw is a paired bone. Each half has a body and four processes: frontal, zygomatic, palatine and alveolar. The latter ends on the right and left with alveolar tubercles.
The upper jaw is a paired bone. Each half has a body and four processes: frontal, zygomatic, palatine and alveolar. The latter ends on the right and left with alveolar tubercles.


 The alveolar process of the upper or alveolar part of the lower jaw is the part where the roots of the teeth are located.
The alveolar process of the upper or alveolar part of the lower jaw is the part where the roots of the teeth are located.
 The maxillary bones are involved in the formation of the orbits, nasal cavity and infratemporal cavity. There is a sinus inside the body of the jaw.
The maxillary bones are involved in the formation of the orbits, nasal cavity and infratemporal cavity. There is a sinus inside the body of the jaw.
 This structure is due to the functions of breathing, speech production and chewing. At the same time, resistance to chewing pressure on upper jaw provide bone abutments (buttresses).
This structure is due to the functions of breathing, speech production and chewing. At the same time, resistance to chewing pressure on upper jaw provide bone abutments (buttresses).
 Buttresses (French - counteracting force, counter-supports) are powerful thickenings of the compact substance of the upper jaw, which are a means of transmitting chewing pressure.
Buttresses (French - counteracting force, counter-supports) are powerful thickenings of the compact substance of the upper jaw, which are a means of transmitting chewing pressure.

 The chewing pressure emanating from the central, lateral incisors, canine and first premolar is distributed vertically along the frontonasal buttresses to the surface of the orbit, nasal, lacrimal and frontal bones.
The chewing pressure emanating from the central, lateral incisors, canine and first premolar is distributed vertically along the frontonasal buttresses to the surface of the orbit, nasal, lacrimal and frontal bones.

 The zygomaticalveolar ridge, the zygomatic bone with the zygomatic process form the zygomatic buttress, along which the pressure from the lateral teeth is distributed along the lateral edge of the orbit to the frontal bone, through the zygomatic arch to temporal bone, as well as through the lower edge of the orbit into the upper part of the frontonasal buttress.
The zygomaticalveolar ridge, the zygomatic bone with the zygomatic process form the zygomatic buttress, along which the pressure from the lateral teeth is distributed along the lateral edge of the orbit to the frontal bone, through the zygomatic arch to temporal bone, as well as through the lower edge of the orbit into the upper part of the frontonasal buttress.
 Chewing pressure from the lateral teeth is also perceived by the pterygopalatine buttress, formed by the tubercle of the upper jaw and the pterygoid process. It transmits it to the base of the skull.
Chewing pressure from the lateral teeth is also perceived by the pterygopalatine buttress, formed by the tubercle of the upper jaw and the pterygoid process. It transmits it to the base of the skull.
 The palatal buttress balances transverse horizontal stresses. It is formed by the palatine processes of the upper jaw, which make up the hard palate.
The palatal buttress balances transverse horizontal stresses. It is formed by the palatine processes of the upper jaw, which make up the hard palate.
 The hard palate includes the palatine processes of the upper jaw and the horizontal plates of the palatine bone, covered with mucous membrane and submucosal layer.
The hard palate includes the palatine processes of the upper jaw and the horizontal plates of the palatine bone, covered with mucous membrane and submucosal layer.
 The vault of the hard palate can have different heights and configurations. In the area of the median palatal suture, a palatine ridge (torus palatinus) is sometimes identified.
The vault of the hard palate can have different heights and configurations. In the area of the median palatal suture, a palatine ridge (torus palatinus) is sometimes identified.
 The soft palate in front borders on the posterior edge of the hard palate, on the sides it is connected with the lateral walls of the pharynx. Dorsally it ends with a free edge, repeating the configuration of the posterior edge of the bones of the hard palate.
The soft palate in front borders on the posterior edge of the hard palate, on the sides it is connected with the lateral walls of the pharynx. Dorsally it ends with a free edge, repeating the configuration of the posterior edge of the bones of the hard palate.
 The soft palate is formed by a number of muscles: tt. uvulae - muscles of the uvula (shorten the uvula, raising it); tensor veli palatini - a muscle that stretches the soft palate (it tightens the anterior section of the soft palate and the pharyngeal section of the auditory tube); so-called levator veli palatini - muscle that lifts the soft palate (narrows the pharyngeal opening of the auditory tube); t. palatoglossus - palate lingual muscle(narrows the pharynx, bringing the anterior arches closer to the root of the tongue); t. palatopharyngeus - palatopharyngeus muscle (brings together the palatopharyngeal arches and pulls up the lower part of the pharynx and larynx).
The soft palate is formed by a number of muscles: tt. uvulae - muscles of the uvula (shorten the uvula, raising it); tensor veli palatini - a muscle that stretches the soft palate (it tightens the anterior section of the soft palate and the pharyngeal section of the auditory tube); so-called levator veli palatini - muscle that lifts the soft palate (narrows the pharyngeal opening of the auditory tube); t. palatoglossus - palate lingual muscle(narrows the pharynx, bringing the anterior arches closer to the root of the tongue); t. palatopharyngeus - palatopharyngeus muscle (brings together the palatopharyngeal arches and pulls up the lower part of the pharynx and larynx).
 The body passes into the alveolar part, in which the roots of the teeth are located. The branch has two processes: the condylar, ending in the head of the lower jaw, and the coronoid.
The body passes into the alveolar part, in which the roots of the teeth are located. The branch has two processes: the condylar, ending in the head of the lower jaw, and the coronoid.
 The ratio of the height of the branch to the length of the jaw body in adults is 6.5-7:10. The angle of the lower jaw is normally 120 + 5° (V.N. Trezubov).
The ratio of the height of the branch to the length of the jaw body in adults is 6.5-7:10. The angle of the lower jaw is normally 120 + 5° (V.N. Trezubov).
 The lower jaw is covered with a compact plate, which also lines the walls of the dental alveoli. The most massively compact substance is present in the area of the chin, corners and at the base of the jaw. Between the plates of the compact substance there is a spongy bone substance, especially developed in the body and head of the lower jaw.
The lower jaw is covered with a compact plate, which also lines the walls of the dental alveoli. The most massively compact substance is present in the area of the chin, corners and at the base of the jaw. Between the plates of the compact substance there is a spongy bone substance, especially developed in the body and head of the lower jaw.
 The trajectories of the lower jaw are strictly defined locations of the beams of the spongy substance, oriented by the functional load. Inside the lower jaw there are two canals that open into the mental and mandibular foramina.
The trajectories of the lower jaw are strictly defined locations of the beams of the spongy substance, oriented by the functional load. Inside the lower jaw there are two canals that open into the mental and mandibular foramina.
 The temporomandibular joint (TMJ) articulates the lower jaw with the temporal bone. In its structure it is ellipsoidal. His anatomical features are the presence of an articular disc and a discrepancy between the articulating surfaces (incongruence). Functionally, it is a paired joint.
The temporomandibular joint (TMJ) articulates the lower jaw with the temporal bone. In its structure it is ellipsoidal. His anatomical features are the presence of an articular disc and a discrepancy between the articulating surfaces (incongruence). Functionally, it is a paired joint.

 In the joint cavity there is a biconcave oval-shaped cartilaginous plate - the articular disc. It divides the joint cavity into two non-communicating sections: upper and lower. The disc compensates for the discrepancy between the relief of the articular surfaces.
In the joint cavity there is a biconcave oval-shaped cartilaginous plate - the articular disc. It divides the joint cavity into two non-communicating sections: upper and lower. The disc compensates for the discrepancy between the relief of the articular surfaces.

 Chewing muscles – m. masseter - actually chewing; m. temporalis - temporal; – m. pterygoideus medialis - medial pterygoid; – m. pterygoideus lateralis - lateral pterygoid; – m. mylohyoideus - maxillohyoid; – m. geniohyoideus - geniohyoid; – venter anterior t. digastricus - anterior belly of the digastric muscle
Chewing muscles – m. masseter - actually chewing; m. temporalis - temporal; – m. pterygoideus medialis - medial pterygoid; – m. pterygoideus lateralis - lateral pterygoid; – m. mylohyoideus - maxillohyoid; – m. geniohyoideus - geniohyoid; – venter anterior t. digastricus - anterior belly of the digastric muscle



 When they contract, the masticatory muscles move lower jaw in different directions, thus participating in the act of chewing, swallowing, sound production, and speech.
When they contract, the masticatory muscles move lower jaw in different directions, thus participating in the act of chewing, swallowing, sound production, and speech.
 In accordance with the main directions of their action, the masticatory muscles are divided into three groups: – the first includes the muscles that lower the lower gelus (m. mylohyoideus, i.e. geniohyoideus, venter anterior i. digastricus); – the second group includes the muscles that lift the inferior gelus (w. masseter, m. temporalis, m. pterygoideus medialis); – the third group is the paired lateral pterygoid muscle (m. pterygoideus lateralis). With their synchronous contraction, the lower jaw moves forward; with unilateral contraction of the muscle, the lower jaw moves in the opposite direction. Thus, the muscles of the third group provide anterior and lateral movements of the lower gel.
In accordance with the main directions of their action, the masticatory muscles are divided into three groups: – the first includes the muscles that lower the lower gelus (m. mylohyoideus, i.e. geniohyoideus, venter anterior i. digastricus); – the second group includes the muscles that lift the inferior gelus (w. masseter, m. temporalis, m. pterygoideus medialis); – the third group is the paired lateral pterygoid muscle (m. pterygoideus lateralis). With their synchronous contraction, the lower jaw moves forward; with unilateral contraction of the muscle, the lower jaw moves in the opposite direction. Thus, the muscles of the third group provide anterior and lateral movements of the lower gel.
 Facial muscles of the lower part of the face: m. orbicularis oris - orbicularis oris muscle; m levator labii superioris - muscle that lifts the upper lip; m. depressor labii interioris - depressor muscle lower lip; m. buccinator - buccal muscle; m. zygomaticus major - zygomaticus major muscle; m. levator anguli oris - muscle that lifts the angle of the mouth; m. depressor anguli oris - muscle that lowers the angle of the mouth; m. risorius - muscle of laughter; m. mentalis - mentalis muscle; m. incisivus labii superioris - incisor muscle upper lip; m. incisivus labii inferioris - incisor muscle of the lower lip.
Facial muscles of the lower part of the face: m. orbicularis oris - orbicularis oris muscle; m levator labii superioris - muscle that lifts the upper lip; m. depressor labii interioris - depressor muscle lower lip; m. buccinator - buccal muscle; m. zygomaticus major - zygomaticus major muscle; m. levator anguli oris - muscle that lifts the angle of the mouth; m. depressor anguli oris - muscle that lowers the angle of the mouth; m. risorius - muscle of laughter; m. mentalis - mentalis muscle; m. incisivus labii superioris - incisor muscle upper lip; m. incisivus labii inferioris - incisor muscle of the lower lip.

 Chewing pressure The absolute strength of the masticatory muscles is the tension developed by the masticatory muscle during its maximum contraction. The absolute strength of the masticatory muscles, according to various sources, ranges from 80 to 390 kg.
Chewing pressure The absolute strength of the masticatory muscles is the tension developed by the masticatory muscle during its maximum contraction. The absolute strength of the masticatory muscles, according to various sources, ranges from 80 to 390 kg.
 Chewing pressure is the force developed by the masticatory muscles and regulated by periodontal receptors, necessary for crushing, biting, and crushing food. Chewing pressure on the incisors is approximately equal in women - 20-30 kg, in men - 25-40 kg, on molars, respectively - 40-60 kg and 50-80 kg.
Chewing pressure is the force developed by the masticatory muscles and regulated by periodontal receptors, necessary for crushing, biting, and crushing food. Chewing pressure on the incisors is approximately equal in women - 20-30 kg, in men - 25-40 kg, on molars, respectively - 40-60 kg and 50-80 kg.
 TEETH AND DENTAL ARCHES (DENTAL ARCHES) Dental organs are an integral part of the chewing vocal apparatus. The latter contains 32 dental organs, 16 each on the upper and lower jaws.
TEETH AND DENTAL ARCHES (DENTAL ARCHES) Dental organs are an integral part of the chewing vocal apparatus. The latter contains 32 dental organs, 16 each on the upper and lower jaws.
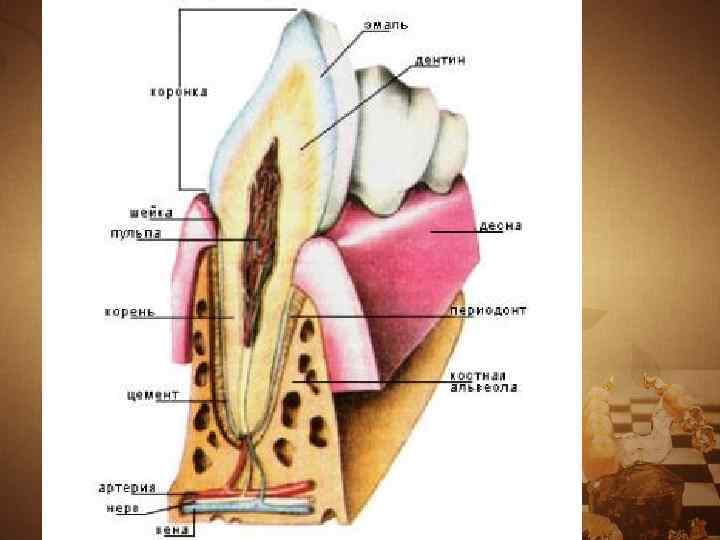
 Each dental organ consists of: – a tooth; – the socket and the adjacent part of the jaw, covered with the mucous membrane of the gums; – ligamentous complex (periodontal) that holds the tooth in the socket; – blood vessels and nerves.
Each dental organ consists of: – a tooth; – the socket and the adjacent part of the jaw, covered with the mucous membrane of the gums; – ligamentous complex (periodontal) that holds the tooth in the socket; – blood vessels and nerves.

 Dental organ = tooth + periodontium. Tooth (Latin - dens, Gr - odus) is a very dense, hollow, elongated rod used for biting, crushing, grinding and grinding solid food.
Dental organ = tooth + periodontium. Tooth (Latin - dens, Gr - odus) is a very dense, hollow, elongated rod used for biting, crushing, grinding and grinding solid food.
 In practical dentistry, it is customary to distinguish between anatomical and clinical crowns. – Anatomical crown is the part of the tooth covered with enamel. – Clinical crown is the part of the tooth protruding above the gum.
In practical dentistry, it is customary to distinguish between anatomical and clinical crowns. – Anatomical crown is the part of the tooth covered with enamel. – Clinical crown is the part of the tooth protruding above the gum.
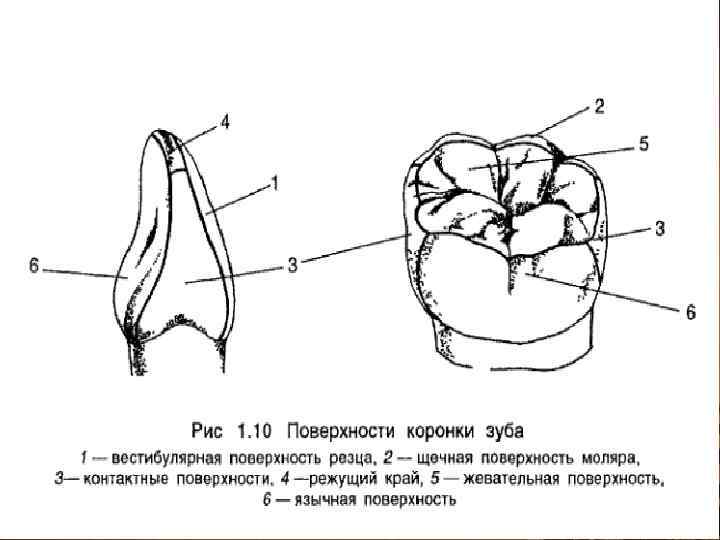
 The following surfaces are distinguished on the crown of the tooth: 1) the surface facing the vestibule of the oral cavity is called vestibular. In the front teeth it is also called the labial surface, and in the lateral teeth - the buccal surface; 2) the surface of the tooth crown facing the oral cavity is called oral, or oral. On the upper jaw it is called palatine, and on the lower jaw it is called lingual;
The following surfaces are distinguished on the crown of the tooth: 1) the surface facing the vestibule of the oral cavity is called vestibular. In the front teeth it is also called the labial surface, and in the lateral teeth - the buccal surface; 2) the surface of the tooth crown facing the oral cavity is called oral, or oral. On the upper jaw it is called palatine, and on the lower jaw it is called lingual;
 3) the surfaces of the crown facing the adjacent teeth of their row are called contact. The surfaces of the teeth facing the center of the dentition are called mesial contact, on the central incisors - medial. Surfaces directed in the opposite direction, i.e., from the center of the dentition, are called distal contact;
3) the surfaces of the crown facing the adjacent teeth of their row are called contact. The surfaces of the teeth facing the center of the dentition are called mesial contact, on the central incisors - medial. Surfaces directed in the opposite direction, i.e., from the center of the dentition, are called distal contact;
 4) the surface or edge of the tooth crown directed towards the teeth of the opposite dentition is called the chewing surface or chewing (cutting) edge of the incisors and canines. It is also called the closure surface or occlusal surface, because it comes into contact with the teeth of the opposite dentition when the jaws approach.
4) the surface or edge of the tooth crown directed towards the teeth of the opposite dentition is called the chewing surface or chewing (cutting) edge of the incisors and canines. It is also called the closure surface or occlusal surface, because it comes into contact with the teeth of the opposite dentition when the jaws approach.
 The cavity of the tooth has different shape V different teeth. Inside the crown, the tooth cavity is somewhat similar in shape to it, and at the root continues in the form of a canal. The latter ends with a small hole at the top of the tooth root. In multi-rooted teeth, the number of root canals is usually equal to the number of roots.
The cavity of the tooth has different shape V different teeth. Inside the crown, the tooth cavity is somewhat similar in shape to it, and at the root continues in the form of a canal. The latter ends with a small hole at the top of the tooth root. In multi-rooted teeth, the number of root canals is usually equal to the number of roots.
 The tooth cavity is filled with dental pulp - pulp. The latter distinguishes between the crown and root parts. Vessels and nerves enter the pulp through the opening of the root apex.
The tooth cavity is filled with dental pulp - pulp. The latter distinguishes between the crown and root parts. Vessels and nerves enter the pulp through the opening of the root apex.
 Dental pulp - dental pulp, loose connective tissue, rich in blood vessels and nerves, filling the tooth cavity. The pulp performs: trophic, plastigetic (dentin-forming), protective functions.
Dental pulp - dental pulp, loose connective tissue, rich in blood vessels and nerves, filling the tooth cavity. The pulp performs: trophic, plastigetic (dentin-forming), protective functions.
 The main dental tissue - dentin - consists of a basic substance impregnated with lime salts, and large quantity tubes (tubules). – Dentin is the hard part of the tooth, similar to bone, surrounding the tooth cavity and root canals.
The main dental tissue - dentin - consists of a basic substance impregnated with lime salts, and large quantity tubes (tubules). – Dentin is the hard part of the tooth, similar to bone, surrounding the tooth cavity and root canals.
 Dentin is 5-6 times harder than bone. Its main substance includes collagen fibers and the substance connecting them. Dentin contains about 70-72% mineral salts, and the rest consists of organic matter, fat and water. The salts contain the most hydroxyapatite [Ca 3 (P 04) 2 × Ca (OH) 2].
Dentin is 5-6 times harder than bone. Its main substance includes collagen fibers and the substance connecting them. Dentin contains about 70-72% mineral salts, and the rest consists of organic matter, fat and water. The salts contain the most hydroxyapatite [Ca 3 (P 04) 2 × Ca (OH) 2].
 Enamel is the hard tissue of the tooth that covers the outside of the dentin of the crown. Enamel contains 96-97% mineral salts and only 3-4% comes from organic matter. Among the salts, hydroxyapatite predominates (84%). In addition to it, the enamel contains calcium carbonate, calcium fluoride and magnesium phosphate.
Enamel is the hard tissue of the tooth that covers the outside of the dentin of the crown. Enamel contains 96-97% mineral salts and only 3-4% comes from organic matter. Among the salts, hydroxyapatite predominates (84%). In addition to it, the enamel contains calcium carbonate, calcium fluoride and magnesium phosphate.
 The cementum covers the dentin of the root and in its structure resembles coarse-fibered bone. Cementum is a dense tissue resembling coarse-fibered bone that covers the outside of the dentin of the tooth root. By chemical composition it is similar to dentin, but contains slightly more organic substances and only 60% inorganic.
The cementum covers the dentin of the root and in its structure resembles coarse-fibered bone. Cementum is a dense tissue resembling coarse-fibered bone that covers the outside of the dentin of the tooth root. By chemical composition it is similar to dentin, but contains slightly more organic substances and only 60% inorganic.
 The dental organs in the jaws are located so that the crowns of the teeth form the dentition - upper and lower. The adult dentition includes 16 teeth. In the center of the dentition there are teeth that bite, and on the sides there are teeth that grind and crush food.
The dental organs in the jaws are located so that the crowns of the teeth form the dentition - upper and lower. The adult dentition includes 16 teeth. In the center of the dentition there are teeth that bite, and on the sides there are teeth that grind and crush food.

 The dental arch is an imaginary curve passing along the cutting edge and the middle of the chewing surface of the dentition. The upper dentition of permanent teeth has the shape of a semi-ellipse, and the lower one - a parabola.
The dental arch is an imaginary curve passing along the cutting edge and the middle of the chewing surface of the dentition. The upper dentition of permanent teeth has the shape of a semi-ellipse, and the lower one - a parabola.
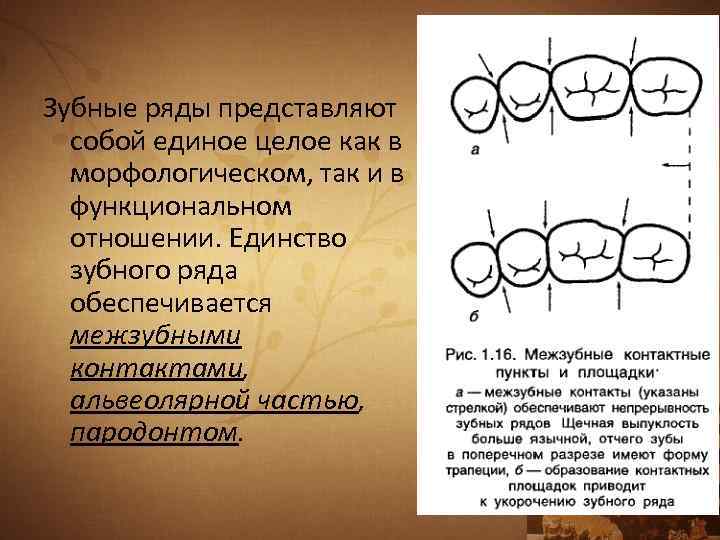 The dentition is a single whole, both morphologically and functionally. The unity of the dentition is ensured by interdental contacts, the alveolar part, and periodontium.
The dentition is a single whole, both morphologically and functionally. The unity of the dentition is ensured by interdental contacts, the alveolar part, and periodontium.
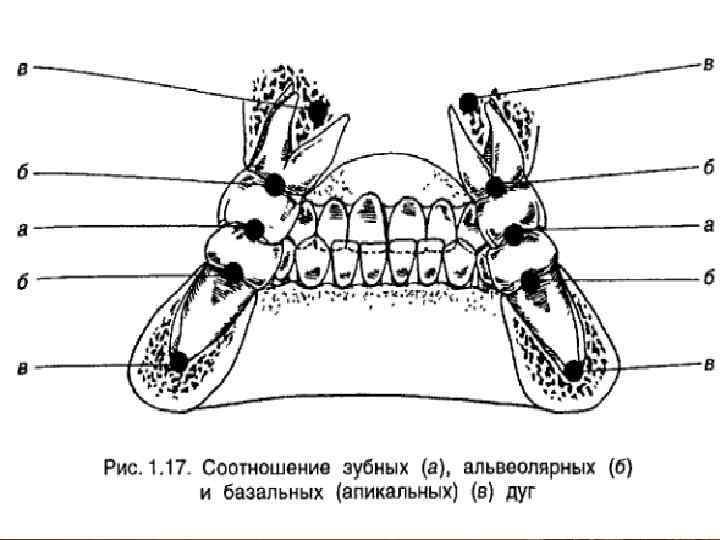
 IN orthopedic dentistry It is customary to distinguish, in addition to the dental arch, the alveolar and basal (apical) arches. The alveolar arch refers to an imaginary line drawn along the middle of the alveolar ridge. The basal arch is an imaginary curve that runs along the tops of the roots of the teeth. Often called the apical base.
IN orthopedic dentistry It is customary to distinguish, in addition to the dental arch, the alveolar and basal (apical) arches. The alveolar arch refers to an imaginary line drawn along the middle of the alveolar ridge. The basal arch is an imaginary curve that runs along the tops of the roots of the teeth. Often called the apical base.
 STRUCTURE AND FUNCTIONS OF PERIODONTAL periodontium is the supporting system of teeth. Includes: periodontium, gums, dental alveoli, tooth root cement.
STRUCTURE AND FUNCTIONS OF PERIODONTAL periodontium is the supporting system of teeth. Includes: periodontium, gums, dental alveoli, tooth root cement.

 Periodontium is dense connective tissue. Of greatest interest is its main substance with functionally oriented connective tissue fibers.
Periodontium is dense connective tissue. Of greatest interest is its main substance with functionally oriented connective tissue fibers.
 Functions of the periodontium: supporting support, carried out by the periodontal ligament complex, gum and alveolus; trophic, caused by hydraulic pressure on the network of blood vessels and lymphatic vessels carried out by the root during chewing microexcursions of the tooth; shock-absorbing, which consists in crushing chewing pressure and extinguishing the amplitude of microexcursions of the tooth; sensory, regulating chewing pressure and implemented by the periodontal receptor system; plastiges - bone and cement-forming.
Functions of the periodontium: supporting support, carried out by the periodontal ligament complex, gum and alveolus; trophic, caused by hydraulic pressure on the network of blood vessels and lymphatic vessels carried out by the root during chewing microexcursions of the tooth; shock-absorbing, which consists in crushing chewing pressure and extinguishing the amplitude of microexcursions of the tooth; sensory, regulating chewing pressure and implemented by the periodontal receptor system; plastiges - bone and cement-forming.
 OCCLUSAL SURFACE OF DENTAL RANKS The occlusal surface of the dentition is the totality of the occlusal surfaces of all teeth included in it.
OCCLUSAL SURFACE OF DENTAL RANKS The occlusal surface of the dentition is the totality of the occlusal surfaces of all teeth included in it.
 Schematically, the occlusal surface in the lateral projection is depicted as a curve passing from the cutting edges of the central incisors to the distal cusps of the third molars. This occlusal curve is called the sagittal curve. It is convexly directed downward.
Schematically, the occlusal surface in the lateral projection is depicted as a curve passing from the cutting edges of the central incisors to the distal cusps of the third molars. This occlusal curve is called the sagittal curve. It is convexly directed downward.
 In addition to the sagittal occlusal curve, a transversal occlusal curve is distinguished. It passes through the chewing surfaces of the molars of the right and left sides in the transverse direction.
In addition to the sagittal occlusal curve, a transversal occlusal curve is distinguished. It passes through the chewing surfaces of the molars of the right and left sides in the transverse direction.
 The occlusal plane is an imaginary plane drawn in two ways. In the first case, it passes through the middle of the overlap of the central incisors and the middle of the overlap of the mesial cusps of the first (in their absence, the second) molars. In the second option, it is carried out through the apices of the buccal cusp of the second upper premolar and the mesial buccal cusp of the first upper molar. The plane formed during prosthetics on the occlusal ridges is also called prosthetic.
The occlusal plane is an imaginary plane drawn in two ways. In the first case, it passes through the middle of the overlap of the central incisors and the middle of the overlap of the mesial cusps of the first (in their absence, the second) molars. In the second option, it is carried out through the apices of the buccal cusp of the second upper premolar and the mesial buccal cusp of the first upper molar. The plane formed during prosthetics on the occlusal ridges is also called prosthetic.
 OCCLUSION, ARTICULATION Occlusion (from the Latin occlusus - locked) is the closure of the dentition or individual groups of antagonist teeth.
OCCLUSION, ARTICULATION Occlusion (from the Latin occlusus - locked) is the closure of the dentition or individual groups of antagonist teeth.
 Articulation (from the Latin articulatio - articulation) - all kinds of positions and movements of the lower jaw in relation to the upper, carried out with the help of the masticatory muscles. Articulation is a chain of successive occlusions.
Articulation (from the Latin articulatio - articulation) - all kinds of positions and movements of the lower jaw in relation to the upper, carried out with the help of the masticatory muscles. Articulation is a chain of successive occlusions.
 There are five main types of occlusion: – central; – front; – lateral (right and left); - back.
There are five main types of occlusion: – central; – front; – lateral (right and left); - back.
 Central occlusion is a closure of the dentition in which there is a maximum number of interdental contacts. The head of the lower jaw is located at the base of the slope of the articular tubercle, and the muscles that bring the lower row of teeth into contact with the upper row (temporal, chewing, medial pterygoid) are simultaneously and evenly contracted. From this position, lateral shifts of the lower jaw are still possible.
Central occlusion is a closure of the dentition in which there is a maximum number of interdental contacts. The head of the lower jaw is located at the base of the slope of the articular tubercle, and the muscles that bring the lower row of teeth into contact with the upper row (temporal, chewing, medial pterygoid) are simultaneously and evenly contracted. From this position, lateral shifts of the lower jaw are still possible.
 Anterior occlusion is characterized by protrusion of the lower jaw forward. This is achieved by bilateral contraction of the lateral pterygoid muscles. With a normal bite, the midline of the face, as with central occlusion, coincides with the midline passing between the incisors. The heads of the lower jaw are shifted forward and located closer to the top of the articular tubercles.
Anterior occlusion is characterized by protrusion of the lower jaw forward. This is achieved by bilateral contraction of the lateral pterygoid muscles. With a normal bite, the midline of the face, as with central occlusion, coincides with the midline passing between the incisors. The heads of the lower jaw are shifted forward and located closer to the top of the articular tubercles.
 Lateral occlusion occurs when the lower jaw moves to the right (right lateral occlusion) or to the left (left lateral occlusion). The head of the lower jaw on the side of the displacement, rotating slightly, remains at the base of the articular tubercle, and on the opposite side it moves to the top of the articular tubercle. Lateral occlusion is accompanied by unilateral contraction of the lateral pterygoid muscle opposite to the displacement of the side.
Lateral occlusion occurs when the lower jaw moves to the right (right lateral occlusion) or to the left (left lateral occlusion). The head of the lower jaw on the side of the displacement, rotating slightly, remains at the base of the articular tubercle, and on the opposite side it moves to the top of the articular tubercle. Lateral occlusion is accompanied by unilateral contraction of the lateral pterygoid muscle opposite to the displacement of the side.
 Pathological occlusion is the closure of teeth, in which there is a violation of the shape and function of the masticatory apparatus. This occlusion is observed with partial loss of teeth, anomalies, deformations, periodontal diseases, and increased tooth wear. With pathological occlusion, functional overload of the periodontium, masticatory muscles, temporomandibular joints, and blockade of mandibular movements may occur.
Pathological occlusion is the closure of teeth, in which there is a violation of the shape and function of the masticatory apparatus. This occlusion is observed with partial loss of teeth, anomalies, deformations, periodontal diseases, and increased tooth wear. With pathological occlusion, functional overload of the periodontium, masticatory muscles, temporomandibular joints, and blockade of mandibular movements may occur.
 FEATURES OF THE STRUCTURE OF THE ORAL MUCOSA, HAVING APPLIED SIGNIFICANCE In dentistry, a distinction is made between mobile and immobile mucous membrane. The basis for the mobility and immobility of the oral mucosa is the presence or absence of the submucosa (tela submucosa).
FEATURES OF THE STRUCTURE OF THE ORAL MUCOSA, HAVING APPLIED SIGNIFICANCE In dentistry, a distinction is made between mobile and immobile mucous membrane. The basis for the mobility and immobility of the oral mucosa is the presence or absence of the submucosa (tela submucosa).
 The mobile mucous membrane makes excursions when the facial muscles contract. Such mobility is called active, and the mucous membrane that has it is called actively mobile. The immobile mucous membrane does not have this ability. It most often covers the tops of the alveolar ridges, the anterior third of the hard palate and its middle part.
The mobile mucous membrane makes excursions when the facial muscles contract. Such mobility is called active, and the mucous membrane that has it is called actively mobile. The immobile mucous membrane does not have this ability. It most often covers the tops of the alveolar ridges, the anterior third of the hard palate and its middle part.
 When the mucous membrane passes from the alveolar process to the lip and cheeks, the arch of the vestibule is formed. An imaginary line drawn along the top of the arch of the vestibule of the oral cavity is called a transitional fold.
When the mucous membrane passes from the alveolar process to the lip and cheeks, the arch of the vestibule is formed. An imaginary line drawn along the top of the arch of the vestibule of the oral cavity is called a transitional fold. 
Slide 2
An organ (from the gr.organon - tool, instrument, organ) is a phylogenetically formed complex of various tissues, united by development, general structure and function. An organ is an integral formation that has a certain form, structure, function, development and position in the body that is unique to it.
Slide 3
System (from gr.systema - a whole made up of parts; connection) - a set of organs that are similar in their general structure, function, origin and development. The dentition forms a single functional system - the dentofacial system, the unity and stability of which is ensured by the alveolar process of the upper and alveolar parts of the lower jaw, and periodontium.
Slide 4
Apparatus (from Latin apparatus) is a union of systems and individual organs that function in a similar direction or have a common origin and location.
Slide 5
The chewing-speech apparatus is a complex of interconnected and interacting systems and individual organs involved in chewing, breathing, sound production and speech.
Slide 6
The masticatory-speech apparatus includes: the facial skeleton and temporomandibular joints; chewing muscles; organs intended for grasping, moving food, forming a bolus of food, for swallowing, as well as the sound-speech system: lips, cheeks with their facial muscles, palate, tongue; organs for biting, crushing and grinding food (teeth), and its enzymatic processing (salivary glands).
Slide 7
Upper jaw
The upper jaw is a paired bone. Each half has a body and four processes: frontal, zygomatic, palatine and alveolar. The latter ends on the right and left with alveolar tubercles.
Slide 8
Slide 9
Slide 10
The alveolar process of the upper or alveolar part of the lower jaw is the part where the roots of the teeth are located.
Slide 11
The maxillary bones are involved in the formation of the orbits, nasal cavity and infratemporal cavity. There is a sinus inside the body of the jaw.
Slide 12
This structure is due to the functions of breathing, speech production and chewing. In this case, resistance to chewing pressure on the upper jaw is provided by bone abutments (buttresses).
Slide 13
Buttresses (fr. - counteracting force, counter-supports) are powerful thickenings of the compact substance of the upper jaw, which are a means of transmitting chewing pressure.
Slide 14
The following buttresses are distinguished: - frontonasal, - zygomatic, - pterygopalatine, - palatine.
Slide 15
Slide 16
The chewing pressure emanating from the central, lateral incisors, canine and first premolar is distributed vertically along the frontonasal buttresses to the surface of the orbit, nasal, lacrimal and frontal bones.
Slide 17
Slide 18
The zygomaticalveolar ridge, the zygomatic bone with the zygomatic process form the zygomatic buttress, along which pressure from the lateral teeth is distributed along the lateral edge of the orbit to the frontal bone, through the zygomatic arch to the temporal bone, and also through the lower edge of the orbit to the upper part of the frontonasal buttress.
Slide 19
Chewing pressure from the lateral teeth is also perceived by the pterygopalatine buttress, formed by the tubercle of the upper jaw and the pterygoid process. It transmits it to the base of the skull.
Slide 20
The palatal buttress balances transverse horizontal stresses. It is formed by the palatine processes of the upper jaw, which make up the hard palate.
Slide 21
The hard palate includes the palatine processes of the upper jaw and the horizontal plates of the palatine bone, covered with mucous membrane and submucosal layer.
Slide 22
The vault of the hard palate can have different heights and configurations. In the area of the median palatal suture, a palatine ridge (torus palatinus) is sometimes identified.
Slide 23
The soft palate in front borders on the posterior edge of the hard palate, on the sides it is connected with the lateral walls of the pharynx. Dorsally, it ends with a free edge, repeating the configuration of the posterior edge of the bones of the hard palate.
Slide 24
The soft palate is formed by a number of muscles: tt. uvulae - muscles of the uvula (shorten the uvula, raising it); t. tensor veli palatini - muscle that stretches the soft palate (stretches the anterior section of the soft palate and the pharyngeal section of the auditory tube); t. levator veli palatini - muscle that lifts the soft palate (narrows the pharyngeal opening of the auditory tube); t. palatoglossus - palatoglossus muscle (narrows the pharynx, bringing the anterior arches closer to the root of the tongue); t. palatopharyngeus - palatopharyngeal muscle (brings together the palatopharyngeal arches and pulls up the lower part of the pharynx and larynx).
Slide 25
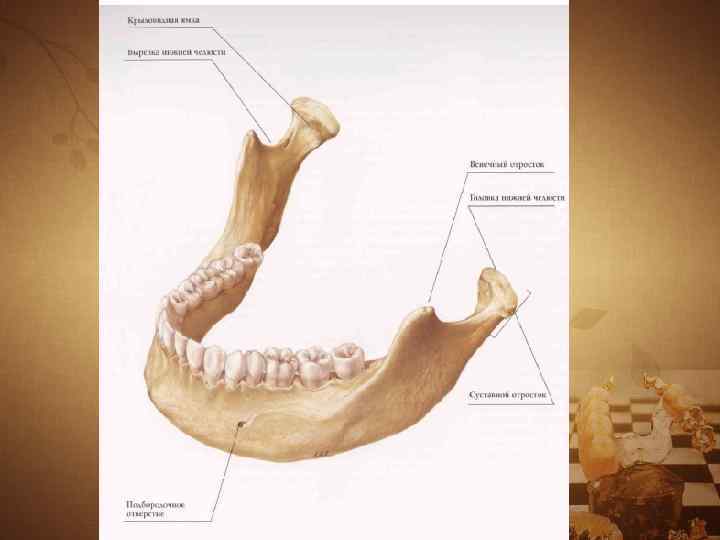
Lower jaw
The lower jaw is a movable bone of the facial skeleton, consisting of a body, a branch, and an angle.
Slide 26
The body passes into the alveolar part, in which the roots of the teeth are located. The branch has two processes - the condylar, ending in the head of the lower jaw, and the coronoid.
Slide 27
Slide 28
The ratio of the height of the branch to the length of the body of the jaw in adults is 6.5-7:10. The angle of the lower jaw is normally 120 + 5° (V.N. Trezubov).
Slide 29
The lower jaw is covered with a compact plate, which also lines the walls of the dental alveoli. The most massively compact substance is present in the area of the chin, corners and at the base of the jaw. Between the plates of the compact substance there is a spongy bone substance, especially developed in the body and head of the lower jaw.
Slide 30
The trajectories of the lower jaw are strictly defined locations of the beams of the spongy substance, oriented by the functional load. Inside the lower jaw there are two canals that open into the mental and mandibular foramina.
Slide 31
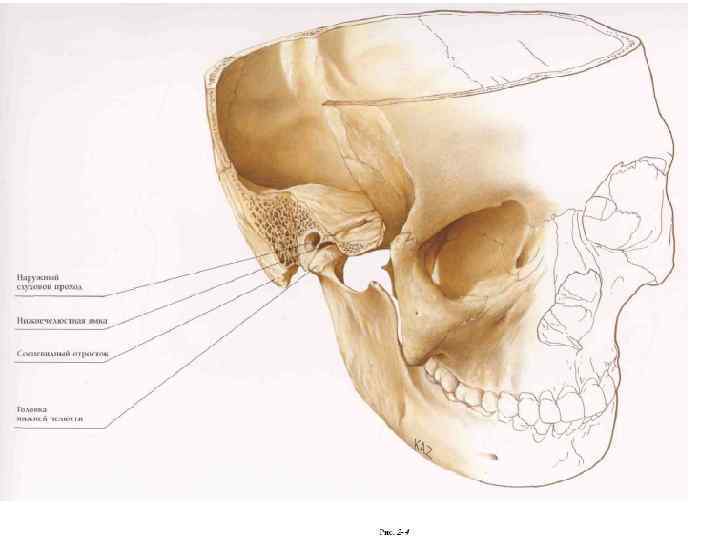
Temporomandibular joint
The temporomandibular joint (TMJ) articulates the lower jaw with the temporal bone. In its structure it is ellipsoidal. Its anatomical features are the presence of an articular disc and a discrepancy between the articulating surfaces (incongruence). Functionally, it is a paired joint.
Slide 32
The joint is formed by the head of the lower jaw, the mandibular fossa and the articular tubercle of the temporal bone.
Slide 33
In the joint cavity there is a biconcave oval-shaped cartilaginous plate - an articular disc. It divides the joint cavity into two non-communicating sections: upper and lower. The disc compensates for the discrepancy between the relief of the articular surfaces.
Slide 34
Slide 35
MUSCLES, MUSCLE STRENGTH, CHEWING PRESSURE
The muscles of the head are divided into: - chewing; - facial expressions.
Slide 36
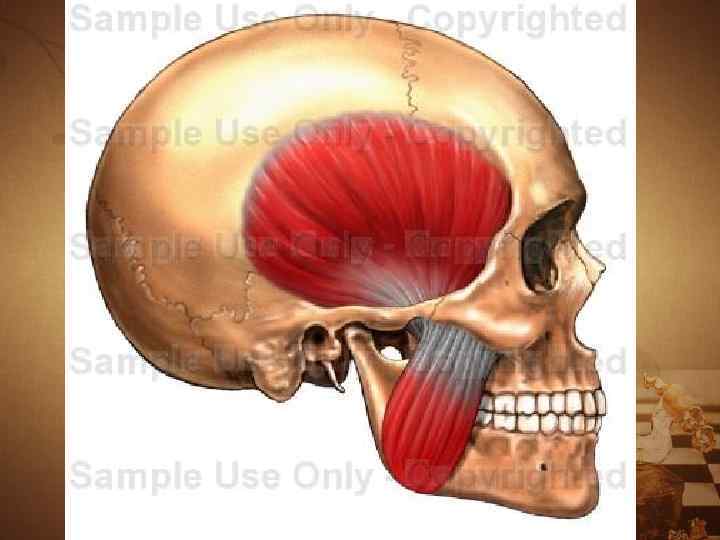
Chewing muscles
m. masseter - actually chewing; m. temporalis - temporal; m. pterygoideus medialis - medial pterygoid; m. pterygoideus lateralis - lateral pterygoid; m. mylohyoideus - mylohyoid; m. geniohyoideus - geniohyoid; venter anterior t. digastricus - anterior belly of the digastric muscle
Slide 37
Slide 38
Slide 39
Slide 40
Slide 41
When they contract, the masticatory muscles move the lower jaw in different directions, thus participating in the act of chewing, swallowing, sound production, and speech.
Slide 42
In accordance with the main directions of their action, the masticatory muscles are divided into three groups: the first includes the muscles that lower the lower gelus (m. mylohyoideus, i.e. geniohyoideus, venter anterior i. digastricus); the second group includes the muscles that lift the inferior gelus (w. masseter, m. temporalis, m. pterygoideus medialis); the third group is the paired lateral pterygoid muscle (m. pterygoideus lateralis). With their synchronous contraction, the lower jaw moves forward; with unilateral contraction of the muscle, the lower jaw moves in the opposite direction. Thus, the muscles of the third group provide anterior and lateral movements of the lower gel.
Slide 43
Facial muscles
Facial muscles of the lower part of the face: m. orbicularis oris - orbicularis oris muscle; m levator labii superioris - muscle that lifts the upper lip; m. depressor labii interioris - muscle that lowers the lower lip; m. buccinator - buccal muscle; m. zygomaticus major - zygomaticus major muscle; m. levator anguli oris - muscle that lifts the angle of the mouth; m. depressor anguli oris - muscle that lowers the angle of the mouth; m. risorius - muscle of laughter; m. mentalis - mentalis muscle; m. incisivus labii superioris - incisor muscle of the upper lip; m. incisivus labii inferioris - incisor muscle of the lower lip.
Slide 44
Slide 45
Chewing pressure
The absolute strength of the masticatory muscles is the tension developed by the masticatory muscle during its maximum contraction. The absolute strength of the masticatory muscles, according to various sources, ranges from 80 to 390 kg.
Slide 46
Chewing pressure is the force developed by the masticatory muscles and regulated by periodontal receptors, necessary for crushing, biting, and crushing food. Chewing pressure on the incisors is approximately equal in women - 20-30 kg, in men - 25-40 kg, on molars, respectively - 40-60 kg and 50-80 kg.
Slide 47
TEETH AND DENTAL ARCHES (DENTAL ARCHES)
The dental organs are an integral part of the chewing-speech apparatus. The latter contains 32 dental organs, 16 each on the upper and lower jaws.
Slide 48
Each dental organ consists of: a tooth; the socket and the adjacent part of the jaw, covered with the mucous membrane of the gums; ligamentous complex (periodontal) that holds the tooth in the socket; vessels and nerves.
Slide 49
Slide 50
Dental organ = tooth + periodontium. Tooth (lat. - dens, gr - odus) is a very dense, hollow, elongated rod used for biting, crushing, grinding and grinding solid food.
Slide 51
In practical dentistry, it is customary to distinguish between anatomical and clinical crowns. Anatomical crown is the part of the tooth covered with enamel. The clinical crown is the part of the tooth that protrudes above the gum.
Slide 52
The following surfaces are distinguished on the crown of the tooth: the surface facing the vestibule of the oral cavity is called vestibular. In the front teeth it is also called the labial surface, and in the lateral teeth - the buccal surface; The surface of the tooth crown facing the oral cavity is called oral, or oral. On the upper jaw it is called palatine, and on the lower jaw it is called lingual;
Slide 53
3) the surfaces of the crown facing the adjacent teeth of their row are called contact. The surfaces of the teeth facing the center of the dentition are called mesial contact, on the central incisors - medial. Surfaces directed in the opposite direction, i.e., from the center of the dentition, are called distal contact;
Slide 54
4) the surface or edge of the tooth crown directed towards the teeth of the opposite dentition is called the chewing surface or chewing (cutting) edge of the incisors and canines. It is also called the closure surface or occlusal surface, because it comes into contact with the teeth of the opposite dentition when the jaws approach.
Slide 55
Slide 56
Tooth cavity - has a different shape in different teeth. Inside the crown, the tooth cavity is somewhat similar in shape to it, and at the root continues in the form of a canal. The latter ends with a small hole at the top of the tooth root. In multi-rooted teeth, the number of root canals is usually equal to the number of roots.
Slide 57
The tooth cavity is filled with dental pulp - pulp. The latter distinguishes between the crown and root parts. Vessels and nerves enter the pulp through the opening of the root apex.
Slide 58
Pulp tooth - dental pulp, loose connective tissue, rich in blood vessels and nerves, filling the tooth cavity. The pulp performs: - trophic, - plastigetic (dentin-forming), - protective functions.
Slide 59
The main dental tissue - dentin - consists of a basic substance impregnated with lime salts and a large number of tubes (tubules). Dentin is the hard part of the tooth, similar to bone, surrounding the tooth cavity and root canals.
Slide 60
Dentin is 5-6 times harder than bone. Its main substance includes collagen fibers and the substance connecting them. Dentin contains about 70-72% mineral salts, and the rest consists of organic matter, fat and water. The salts contain the most hydroxyapatite [Ca3(P04)2 × Ca(OH)2].
Slide 61
Enamel is the hard tissue of the tooth that covers the outside of the dentin of the crown. Enamel contains 96-97% mineral salts and only 3-4% is organic matter. Among the salts, hydroxyapatite predominates (84%). In addition to it, the enamel contains calcium carbonate, calcium fluoride and magnesium phosphate.
Slide 62
The cementum covers the dentin of the root and in its structure resembles coarse-fibered bone. Cementum is a dense tissue resembling coarse-fibered bone that covers the outside of the dentin of the tooth root. Its chemical composition is similar to dentin, but contains slightly more organic substances and only 60% inorganic.
Slide 63
Slide 64
The dental organs in the jaws are located so that the crowns of the teeth form the dentition - upper and lower. The adult dentition includes 16 teeth. In the center of the dentition there are teeth that bite, and on the sides there are teeth that grind and crush food.
Slide 65
Its international equivalent is as follows:
Slide 66
The dental arch is an imaginary curve passing along the cutting edge and the middle of the chewing surface of the dentition. The upper dentition of permanent teeth has the shape of a semi-ellipse, and the lower one - a parabola.
Slide 67
The dentition is a single whole, both morphologically and functionally. The unity of the dentition is ensured by interdental contacts, the alveolar part, and periodontium.
Slide 68
In orthopedic dentistry, it is customary to distinguish, in addition to the dental arch, the alveolar and basal (apical) arches. The subalveolar arch refers to an imaginary line drawn along the middle of the alveolar ridge. The basal arch is an imaginary curve that runs along the tips of the roots of the teeth. Often called the apical base.
Slide 69
Slide 70
STRUCTURE AND FUNCTIONS OF PERIODONTAL
The periodontium is the supporting system of the teeth. Includes: - periodontium, - gums, - dental alveoli, - tooth root cement.
Slide 71
Slide 72
Periodontium is dense connective tissue. Of greatest interest is its main substance with functionally oriented connective tissue fibers.
Slide 73
Periodontal functions: supporting and retaining, carried out by the periodontal ligamentous complex, gum and alveolus; trophic, caused by hydraulic pressure on the network of blood and lymphatic vessels carried out by the root during chewing microexcursions of the tooth; shock-absorbing, which consists in crushing chewing pressure and extinguishing the amplitude of microexcursions of the tooth; sensory, regulating chewing pressure and implemented by the periodontal receptor system; plastiges - bone- and cement-forming.
Slide 74
OCCLUSAL SURFACE OF DENTAL AREA
The occlusal surface of the dentition is the totality of the occlusal surfaces of all teeth included in it.
Slide 75
Schematically, the occlusal surface in the lateral projection is depicted as a curve passing from the cutting edges of the central incisors to the distal cusps of the third molars. This occlusal curve is called the sagittal curve. It is convexly directed downward.
Slide 76
In addition to the sagittal occlusal curve, a transversal occlusal curve is distinguished. It passes through the chewing surfaces of the molars of the right and left sides in the transverse direction.
Slide 77
The occlusal plane is an imaginary plane drawn in two ways. In the first case, it passes through the middle of the overlap of the central incisors and the middle of the overlap of the mesial cusps of the first (in their absence, the second) molars. In the second option, it is carried out through the apices of the buccal cusp of the second upper premolar and the mesial buccal cusp of the first upper molar. The plane formed during prosthetics on the occlusal ridges is also called prosthetic.
Slide 78
OCCLUSION, ARTICULATION
Occlusion (from latocclusus - locked) - closure of dentition or individual groups of antagonist teeth.
Slide 79
Articulation (from the Latin articulatio - articulation) - all kinds of positions and movements of the lower jaw in relation to the upper, carried out with the help of the masticatory muscles. Articulation is a chain of successive occlusions.
Slide 80
There are five main types of occlusion: central; front; lateral (right and left); rear
Slide 81
Central occlusion is a closure of the dentition in which there is a maximum number of interdental contacts. The head of the lower jaw is located at the base of the slope of the articular tubercle, and the muscles that bring the lower row of teeth into contact with the upper row (temporal, chewing, medial pterygoid) are simultaneously and evenly contracted. From this position, lateral shifts of the lower jaw are still possible.
Slide 82
Anterior occlusion is characterized by protrusion of the lower jaw forward. This is achieved by bilateral contraction of the lateral pterygoid muscles. With a normal occlusion, the midline of the face, as in central occlusion, coincides with the midline passing between the incisors. The heads of the lower jaw are shifted forward and located closer to the top of the articular tubercles.
Slide 83
Lateral occlusion occurs when the lower jaw moves to the right (right lateral occlusion) or to the left (left lateral occlusion). The head of the lower jaw on the side of the displacement, rotating slightly, remains at the base of the articular tubercle, and on the opposite side it moves to the top of the articular tubercle. Lateral occlusion is accompanied by unilateral contraction of the lateral pterygoid muscle opposite to the displacement of the side.
Protrusion is the vestibular flat position of the crowns of the front teeth, creating their protrusion outward. Retrusion is the vertical position or oral inclination of the crowns of the front teeth.
Slide 88
FEATURES OF THE STRUCTURE OF THE ORAL MUCOSA, HAVING APPLIED SIGNIFICANCE
In dentistry, a distinction is made between mobile and immobile mucous membrane. The basis for the mobility and immobility of the oral mucosa is the presence or absence of the submucosa (tela submucosa).
Slide 89
The mobile mucous membrane makes excursions when the facial muscles contract. Such mobility is called active, and the mucous membrane that has it is actively mobile. The immobile mucous membrane does not have this ability. It most often covers the tops of the alveolar ridges, the anterior third of the hard palate and its middle part.
Organ(Greek - organon - tool, instrument, organ) - a phylogenetically formed complex of various tissues, united by development, general structure and function.
An organ may contain various tissues, often from all four groups, of which one or more predominate and determine its specific structure and function. An organ is an integral formation that has a certain form, structure, function, development and position in the body that is unique to it. To perform a number of functions, only one organ is not enough. Therefore, complexes of organs - systems - arise.
System(Greek - systema - a whole made up of parts; connection) - a set of organs that are similar in their general structure, function, origin and development.
The dentition forms a single functional system - the dentofacial system, the unity and stability of which is ensured by the alveolar process of the upper and alveolar parts of the lower jaw, the periodontium with the apparatus that fixes the teeth. Human teeth are part of the chewing-speech apparatus.
Apparatus(Latin - apparatus) - a union of systems and individual organs that function in a similar direction or have a common origin and location.
Chewing-speech apparatus- a complex of interconnected and interacting systems and individual organs involved in chewing, breathing, sound production and speech.
It includes:
1) facial skeleton and temporomandibular joints;
2) chewing muscles;
3) organs intended for grasping, moving food, forming a bolus of food, for swallowing, as well as the sound-speech system: lips, cheeks with their facial muscles, palate, tongue;
4) organs for biting, crushing and grinding food (teeth), and its enzymatic processing (salivary glands).
Upper jaw is a paired bone. Each half has a body and four processes: frontal, zygomatic, palatine and alveolar. The latter ends on the right and left with alveolar tubercles. The alveolar process of the upper or alveolar part of the lower jaw is the part where the roots of the teeth are located.
Fig.1.1. Buttresses of the upper jaw (according to Walkhoff): a - front view; b- side view; c - palatal buttresses (primate skull)
The maxillary bones are involved in the formation of the orbits, nasal cavity and infratemporal cavity. There is a sinus inside the body of the jaw. The maxillary bones are openwork. This structure is due to the functions of breathing, speech production and chewing. In this case, resistance to chewing pressure on the upper jaw is provided by bone abutments (buttresses) (Fig. 1.1).
Buttress(French - counteracting force, counter-resistance) - a powerful thickening of the compact substance of the upper jaw, which is a means of transmitting chewing pressure.
The following buttresses are distinguished: frontonasal, zygomatic, pterygopalatine, palatine.
The chewing pressure emanating from the central, lateral incisors, canine and first premolar extends along the frontonasal abutments to the surface of the orbit, nasal, lacrimal and frontal bones, vertically.
The zygomaticalveolar ridge, the zygomatic bone with the zygomatic process form the zygomatic buttress, along which pressure from the lateral teeth is distributed along the lateral edge of the orbit to the frontal bone, through the zygomatic arch to the temporal bone, and also through the lower edge of the orbit to the upper part of the frontonasal buttress.
Chewing pressure from the lateral teeth is also perceived by the pterygopalatine buttress, formed by the tubercle of the upper jaw and the pterygoid process of the main bone. It transmits it to the base of the skull.
The palatal buttress balances transverse horizontal stresses. It is formed by the palatine processes of the upper jaw, which make up the hard palate.
In addition, the formations that strengthen the upper jaw and neutralize the pressure that occurs during chewing include the vomer and the medial walls of the maxillary sinuses.
In a newborn, the upper jaw is underdeveloped, short and wide, consisting mainly of the alveolar process with dental follicles located in it. The body of the jaw is small in size, so the rudiments of baby teeth lie directly under the orbits. The hard palate is flat. As the jaw grows, the alveolar process recedes more and more from the orbit, and the palate gradually takes on the shape of a high dome.
The growth of the upper jaw occurs in three directions. Growth in length and width is associated with the growth and development of teeth, while development in height is associated with age-related changes in the maxillary sinus. Until the age of three, this sinus is located above the bottom of the nasal cavity. In childhood, its bottom is located above the rudiments of permanent teeth. It's smooth. With age, the sinus becomes wider, gradually pushing the alveolar process downwards from the bottom of the orbit. At 3-4 years of life, the maxillary sinus passes beyond the boundaries of the canalis infraorbitalis, and posteriorly approaches the alveolus of the first molar. After the eruption of permanent teeth, the maxillary sinus grows in all directions and reaches normal depth.
In clinical anatomy, there are “hard” and “soft palates”. The first includes the palatine processes of the upper jaw and the horizontal plates of the palatine bone, covered with mucous membrane and submucosal layer. Used as a prosthetic bed for extensive tooth loss in the upper jaw. In the anterior part of the palate there are transverse palatal folds, which are involved in rubbing soft food and thereby enhancing taste perception by the tongue receptors.
The vault of the hard palate can have different heights and configurations. In the area of the median palatal suture, a palatine ridge (torus palatinus) is sometimes identified. The most common shapes of the palatine ridge (V.N. Trezubov, 1966): oval; lanceolate; ellipsoidal; rounded; ovoid; with constriction, in the form of an hourglass; irregular shape. In Fig. 1.2, the shapes of the rollers are presented in order of frequency of occurrence.
Closer to the soft palate (vera palatine), two palatine fossae are contoured, which are landmarks in determining the distal border of the removable denture of the upper jaw. The palate contains pain, tactile, mechano- and thermoreceptors.
R  is. 1.2. Contours of the palatine ridges (according to V.N. Trezubov): a) oval; b) lanceolate; c) ellipsoidal; d) round; e) ovoid; e) with a constriction, in the form of an hourglass; g), h) irregular shape
is. 1.2. Contours of the palatine ridges (according to V.N. Trezubov): a) oval; b) lanceolate; c) ellipsoidal; d) round; e) ovoid; e) with a constriction, in the form of an hourglass; g), h) irregular shape
The soft palate in front borders on the posterior edge of the hard palate, on the sides it is connected with the lateral walls of the pharynx. Dorsally, it ends with a free edge, repeating the configuration of the posterior edge of the bones of the hard palate.
The soft palate is formed by a number of muscles:
Mm. uvulae - muscles of the uvula (shorten the uvula, raising it);
M. tensor veli palatini - muscle that stretches the soft palate (stretches the anterior section of the soft palate and the pharyngeal section of the auditory tube);
M. levator veli palatini - muscle that lifts the soft palate (narrows the pharyngeal opening of the auditory tube);
M. palatoglossus - palatoglossus muscle (narrows the pharynx, bringing the anterior arches closer to the root of the tongue);
M. palatopharyngeus - velopharyngeus muscle (brings together the velopharyngeal arches and pulls up the lower part of the pharynx and larynx).
Of these muscles, only the muscles of the uvula end in the palate itself, and the rest, being paired, connect the soft palate with other organs, which makes it possible to change the position and shape according to a particular function:
When the muscles contract, the oral cavity is completely separated from the pharynx;
When breathing through the nose, the soft palate arches down to the back of the tongue, isolating the oral cavity from the pharynx, due to which free breathing is possible when chewing food;
When breathing through the mouth, as well as during the act of swallowing, the soft palate straightens and tightly adjoins the back wall of the pharynx, separating the nasopharynx from the oral part of the pharynx and the oral cavity. At the same time, the muscles soft palate, which are part of the palatoglossal arches, connect to the transverse muscle of the tongue, forming a compressive pharyngeal ring.
Lower jaw is a movable bone of the facial skeleton, consisting of a body, branch, and angle. The body passes into the alveolar part, in which the roots of the teeth are located. The branch has two processes - the condylar, ending in the head of the lower jaw, and the coronoid. The ratio of the height of the branch to the length of the body of the jaw in adults is 6.5-7:10. The angle of the lower jaw is normally 120° ± 5° (V.N. Trezubov).
The newborn's lower jaw has a developed alveolar portion, a narrow strip of bone underneath that represents the body of the jaw. The height of the alveolar part is 8.5 mm, the height of the jaw body is 3-4 mm. In an adult, the height of the alveolar part is 11.5 mm, the height of the jaw body is 18 mm.
The lower jaw is covered with a compact plate, which also lines the walls of the dental alveoli. The most massively compact substance is present in the area of the chin, corners and at the base of the jaw. In addition, on the outer and inner surfaces of the jaw there are folds of the compact substance - the oblique and mylohyoid lines, respectively.
The mylohyoid line is the place of attachment of the muscle of the same name. It can cause difficulties in the prosthetics of end defects and complete loss of teeth in the lower jaw, when it is represented by a sharp plate. When the base of a removable denture puts pressure on this line, the mucous membrane located between them is injured. This causes acute pain. In such cases, it is necessary to isolate the line, and sometimes its surgical smoothing in the distal sections.
M  Between the plates of the compact substance there is a spongy bone substance, especially developed in the body and head of the lower jaw. It has a more finely looped structure than on the upper jaw. In this case, the crossbars of the spongy substance are not located chaotically, but in a certain direction, in the form of trajectories, the orientation of which is functionally determined (Fig. 1.3).
Between the plates of the compact substance there is a spongy bone substance, especially developed in the body and head of the lower jaw. It has a more finely looped structure than on the upper jaw. In this case, the crossbars of the spongy substance are not located chaotically, but in a certain direction, in the form of trajectories, the orientation of which is functionally determined (Fig. 1.3).
Fig.1.3. Trajectories of the lower jaw
The trajectories of the lower jaw are strictly defined locations of the beams of the spongy substance, oriented by the functional load.
Inside the lower jaw there are two canals that open into the mental and mandibular foramina.
On the inner surface of the chin there is a mental spine.
The alveolar parts have a rich blood supply and innervation. Their free edge does not overlap the enamel-cement border of the teeth, not reaching it by 2-3 mm. The alveoli of adjacent teeth are separated by an interdental septum, the apex of which can have different shapes: pointed, dome-shaped and truncated cone.
In the alveolar part, there are external and internal compact plates and the spongy substance located between them. The outer compact plate is located on the vestibular and oral surfaces, and the inner one lines the sockets.
The structure of the alveolar bone during teething differs from its structure at the end of the teething process. During the period of eruption, the tops of the interalveolar septa are cut towards the erupting tooth. In this case, it seems that there is a bone pocket at the crown of the erupted tooth. Compact record in upper section The interalveolar septum on the side facing the erupted tooth is wider. The pattern of the spongy substance is unclear. As the tooth erupts, the cut line at the top of the interalveolar septum decreases and, with the end of eruption, takes on the shape characteristic of a given child.
The rudiments of the permanent incisors (upper and lower) are placed in the jaws in a cross-section, since their crowns are significantly larger in size than their temporary predecessors, and in small children’s jaws there is not enough space for them. In early childhood, this arrangement of incisor primordia is normal. Further, with the growth of the jaws, the rudiments move and are established near the sites of eruption.
The rudiments of the fangs are always located quite deep in the jaw, but with the growth of the jaws they also migrate towards the surface.
The rudiments of the premolars are initially located orally, and only in the subsequent period do they occupy a place between the roots of the primary molars.
Z  molar buds in early period developments are located in the tubercle of the upper jaw and in the branch of the lower jaw. As the jaws grow, the rudiments occupy their permanent position. An exception may be the third permanent molars, which erupt at a time when jaw growth is almost complete, so the lack of space for them is persistent.
molar buds in early period developments are located in the tubercle of the upper jaw and in the branch of the lower jaw. As the jaws grow, the rudiments occupy their permanent position. An exception may be the third permanent molars, which erupt at a time when jaw growth is almost complete, so the lack of space for them is persistent.
Rice. 1.4. Temporomandibular joint:
a - upper joint space; b- lower joint space; V- articular tubercle; G- joint capsule; d- articular disc; e - head of the lower jaw
Temporomandibular joint carries out the articulation of the lower jaw with the temporal bone (Fig. 1.4). In its structure it is ellipsoidal. Its anatomical features are the presence of an articular disc and the discrepancy between the articulating surfaces (incongruence).
Functionally, it is a paired joint, which together represents one combined joint. When moving in the joints, it is possible to lower and raise the lower jaw, move it forward, backward and to the side (to the right or left). In the latter case, the head rotates around a vertical axis in the joint of the opposite side. In this case, independent movements on only one side are impossible, although movements in each joint can occur in different directions.
The shape and function of the joint are determined by the variety of food consumed, the complex nature of the movements of the lower jaw when biting and chewing food, and the participation of the joint in colloquial speech person. The functions of chewing and speech have a formative effect on the temporomandibular joint throughout a person’s life.
The joint is formed by the head of the lower jaw, the mandibular fossa or, as it is more often called, the fossa and the articular tubercle of the temporal bone. The heads of the lower jaw are ridge-shaped. The longitudinal, converging (converging) axes of their continuation intersect at an obtuse angle at the anterior edge of the occipital foramen.
The mandibular fossa is 2.5-3 times larger than the head of the lower jaw, which ensures free movement of the latter. In front it is limited by the articular tubercle, and behind by the tympanic part of the temporal bone.
The articular tubercle, which forms the anterior border of the mandibular fossa, is an outgrowth of the zygomatic arch.
In the joint cavity there is a biconcave oval-shaped cartilaginous plate - the articular disc. It divides the joint cavity into two non-communicating sections: upper and lower. The disc compensates for the discrepancy between the relief of the articular surfaces.
When the mouth opens, when the head of the lower jaw moves to the top of the articular tubercle, the articular disc moves with it, ensuring the dynamic correspondence of the articular surfaces. This occurs due to the fact that the lateral pterygoid muscle, branching into two bundles, is woven into the upper part of the joint capsule, directly connected to the anterior part of the disc, and is attached to the neck of the lower jaw with the lower bundle. When this muscle contracts, the lower jaw and articular disc move synchronously.
The joint capsule is an elastic connective tissue membrane consisting of two layers: outer fibrous and inner synovial. In the space between the posterior wall of the capsule and the tympanic part of the temporal bone there is loose connective tissue, thanks to which the shocks of the head of the mandible are softened and some movement of it backwards is allowed. The joint is divided into capsular and extracapsular ligaments.
Muscles, muscle strength, chewing pressure.
M  The muscles of the head (Fig. 1.5.) are divided into chewing, facial, and lingual.
The muscles of the head (Fig. 1.5.) are divided into chewing, facial, and lingual.
Rice. 1.5. Head muscles (according to I.S. Kudrin):
a: - 1 - m.temporalis; 2 - m.masseter; 3 - m.occipofrontalis; 4 - v.corrugator supercilii; 5 - m.procerus; 6 - m.orbicularis oculi; 7 -m.zygomaticus major; 8 - m. nasalis; 9 - m.orbicularis oris; 10 - m.levator labii superioris; 11 - m.depressor labii inferioris; 12 - m. mentalis; 13 - m. depressor anguli oris; 14 - m.buccinator;
b: - 1 - m.temporalis; 2 - m.pterygoideus lateralis; 3 - m.pterygoideus medialis
Chewing muscles:
m.masseter- actually chewing;
m. temporalis - temporal;
m.pterygoideus medialis- medial pterygoid;
m.pterygoideus lateralis- lateral pterygoid;
m.mylohyoideus- maxillary-hyoid;
m.geniohyoideus- geniohyoid;
venter anterior m. digastricus - anterior belly of the digastric muscle.
When they contract, the masticatory muscles move the lower jaw in different directions, thus participating in the act of chewing, swallowing, sound production, and speech.
In accordance with the main directions of their action, the masticatory muscles are divided into three groups:
The first includes the muscles that lower the lower jaw (m.mylohyoideus, m.geniohyoideus, venter anterior m.digastricus);
The second group includes the muscles that elevate the mandible (m.masseter, m.temporalis, m.pterygoideus medialis);
The third group is the paired lateral pterygoid muscle (m.pterygoideus lateralis). With their synchronous contraction, the lower jaw moves forward; with unilateral contraction of the muscle, the lower jaw moves in the opposite direction. Thus, the muscles of the third group provide anterior and lateral movements of the lower jaw.
Muscles that lower the mandible. The opening of the mouth is carried out due to the contraction of the muscles lying below the hyoid bone, when its position is fixed by the muscles lying above the said bone. The depressor mandibular muscles form the floor of the mouth. Due to the fact that they have two movable attachment points, the floor of the oral cavity formed by them is capable of a large amplitude of excursions, reducing or increasing the volume of the oral cavity, which is important for moving a bolus of food or liquid and performing the act of swallowing.
The basis of the floor of the mouth (diaphragma oris) is made up of two mylohyoid muscles of the same name (m.mylohyoideus), connected by a fibrous suture. With their wide proximal ends, these muscles are attached to the inner surface of the body of the lower jaw, along the mylohyoid lines, from the last molars to the middle of the chin. The distal surfaces of the muscle are attached to the hyoid bone.
The geniohyoid muscles with their proximal ends are attached to the mental spine (spina mentalis) on the inner surface of the chin. The distal ends lie on the anterior surface of the body of the hyoid bone.
The anterior bellies of the digastric muscles (venter anterior m.digastricus) begin from the tendon jumper between the anterior and posterior bellies, which is attached to the hyoid bone. With its proximal end, this part of the muscle is attached to the bilateral cavity located lateral to the mental spine.
Muscles that lift the mandible. The chewing muscle itself (m.masseter) consists of two parts. The superficial bundles have an oblique direction, starting from the zygomatic process of the upper jaw and the zygomatic arch. The bundles of the deep part go more vertically and start from the zygomatic bone and the deep layer of the temporal fascia. The movable end of the masticatory muscle is attached to the masticatory tuberosity of the angle of the lower jaw.
With bilateral contraction of both masticatory muscles, the lower jaw rises upward, with unilateral contraction - outward on the side of the contracted muscle.
The temporal muscle (m. temporalis) is fixed by three bundles, filling the temporal fossa. The fibers of the anterior bundles are inclined forward, the middle ones are located vertically, and the posterior ones have an occipital slope. A powerful tendon of the muscle passes medially from the zygomatic arch and is attached to the coronoid process of the mandible.
When all muscle bundles contract, the lowered lower jaw rises; when the posterior bundles contract, the lower jaw pushed forward returns back or is transferred from the central position to the posterior one.
The medial pterygoid muscle (m.pterygoideus medialis) starts from the pterygoid fossa of the main bone, goes back and down, attaching to the pterygoid tuberosity on the inner surface of the angle of the lower jaw.
With unilateral contraction of the muscle, the lower jaw moves to the side opposite to the contraction; with bilateral contraction, it moves forward and raises the lowered lower jaw.
All muscles of this group are synergists, the main action of which has a resultant directed upward.
Muscles that protract the lower jaw. The extension of the lower jaw occurs when both lateral pterygoid muscles (m.pterygoideus lateralis) are tensed. This muscle begins with two heads - upper and lower. The superior head of the muscle originates from the greater wing of the main bone and is attached to the articular capsule and interarticular cartilaginous disc of the temporomandibular joint. The lower head starts from the outer plate pterygoid process main bone and, going back, is attached to the neck of the condylar process.
When the muscle contracts, it moves the lower jaw in the direction opposite to the contraction. With bilateral contraction, the muscles push the lower jaw forward.
The mutual antagonism and synergism of the above muscles contributes to the possibility of smooth, rational movements of the lower jaw necessary for chewing and speech.
Facial muscles. Here, from the so-called facial muscles, we will consider those that surround the oral cavity and are directly involved in chewing, in particular, in the formation of a food bolus, sound production and breathing.
Facial muscles of the lower face:
m.orbicularis oris- orbicularis oris muscle;
T.levator labii superioris- muscle that lifts the upper lip;
m. depressor labii interioris- muscle that lowers the lower lip;
m. buccinator- buccal muscle;
m. zygomaticusmajor - zygomaticus major muscle;
m. levator anguli oris - muscle that lifts the anguli oris;
m. depressor anguli oris- depressor anguli oris muscle;
m. risorius- laughter muscle;
m. mentalis- mental muscle;
m. incisivus labii superioris- incisor muscle of the upper lip;
m. incisivus labii inferioris- incisor muscle of the lower lip.
The oral fissure is bordered by the orbicularis oris muscle (m.orbicularis oris). Its fibers are located in the thickness of the upper and lower lips. Narrows the mouth opening and pulls the lips forward. Other muscles that form the base of the cheeks are woven into it. Among them is the muscle that lifts the upper lip (m.levator labii superioris), which begins in three bundles: from the frontal process, the lower orbital edge of the upper jaw, and the anterior surface of the zygomatic bone. Raises the upper lip and tightens the wing of the nose.
The muscle that lowers the lower lip (m.depressor labii interioris) - starts from the front surface of the lower jaw, anterior to the mental foramen, goes up and is woven into the skin of the lower lip and chin. Pulls the lower lip down.
The buccal muscle (m.buccinator) starts from the buccal ridge of the lower jaw, the pterygomaxillary suture, as well as the outer surfaces of the upper and lower jaws in the area of the sockets of the second molars. Moving forward, the muscle bundles pass into the upper and lower lips, and are also woven into the skin of the lips, the corner of the mouth and the mucous membrane of the vestibule of the mouth. Pulls the corner of the mouth to the side, with bilateral contraction, stretches the oral fissure, presses the inner surface of the cheeks to the teeth.
The zygomaticus major muscle (m.zygomaticus major) starts from the outer surface of the zygomatic bone, moving downwards and medially, intertwined with the orbicularis oris muscle and the skin of the corner of the mouth. Pulls the corner of the mouth upward and outward.
The muscle that lifts the angle of the mouth (m.levator anguli oris) begins under the infraorbital foramen and, going down, is woven into the skin of the angle of the mouth and its circular muscle. Pulls the corner of the mouth up and out.
The muscle that lowers the angle of the mouth (m.depressor anguli oris) - with a wide base, starts from the anterior surface of the lower jaw, below the mental foramen. Heading upward, the muscle narrows, reaches the corner of the mouth, where part of the tufts are woven into its skin, and partly into the thickness of the upper lip and pulls the corner of the mouth down and out.
The laughter muscle (m.risorius) is unstable, partly a continuation of the platisma bundles. Part of the fasciculus muscle originates from the masticatory fascia and the skin of the nasolabial fold. Going medially, the muscle bundles are woven into the skin of the corner of the mouth. Pulls the corner of the mouth laterally.
The mental muscle (m.mentalis) starts from the socket elevations of the lower incisors, goes down and is woven into the skin of the chin. Pulls the skin of the chin upward, stretches the lower lip.
The incisive muscle of the upper lip (m.incisivus labii superioris) starts from the alveolar elevations of the apices of the lateral incisor and canine, goes down and is woven into the skin of the corner of the mouth and its circular muscle. Pulls the corner of the mouth up and inward.
The incisive muscle of the lower lip (m.incisivus labii inferioris) starts from the alveolar elevations of the lower lateral incisor and canine, goes upward and is woven into the orbicularis oris muscle and the skin of the lower lip, pulling the lower lip down.
Chewing pressure. The absolute strength of the masticatory muscles is the tension developed by the masticatory muscle during its maximum contraction. The absolute strength of the masticatory muscles, according to various sources, ranges from 80 to 390 kg. There is no doubt that the masticatory muscles can develop pressure much greater than that required for chewing food, but such force occurs extremely rarely, in moments of danger or strong emotional stress.
The amount of chewing pressure is controlled and reflexively limited by the baroreceptors of the periodontium, which reacts with pain to excessive contraction of the masticatory muscles and compression of the dentition. This prevents the destruction of tooth crowns.
AND  chewing pressure is the force developed by the masticatory muscles and regulated by periodontal receptors, necessary for crushing, biting, and crushing food.
chewing pressure is the force developed by the masticatory muscles and regulated by periodontal receptors, necessary for crushing, biting, and crushing food.
Chewing pressure on the incisors is approximately equal in women - 20-30 kg, in men - 25-40 kg, on molars, respectively - 40-60 kg and 50-80 kg.
Fig.1.6. Diagram of the dental organ (according to I.S. Kudrin): 1 - enamel; 2-dentin; 3 - cement; 4 - periodontium; 5 - alveolar part; 6 - mucous membrane of the gums; 7 - gingival groove; 8 - root apex hole
In other words, the chewing pressure developed by the muscle does not exhaust all its strength, but means endurance limit of supporting tissues of teeth, which is determined by heredity, gender, age, degree of periodontal training and some other factors.
Teeth and dentition (dental arches).
The dental organs (Fig. 1.6) are an integral part of the chewing-speech apparatus. The latter in adults contains 32 dental organs, 16 each on the upper and lower jaws. In the primary occlusion there are 20 teeth - 2 incisors, 1 canine, 2 molars on one half of the jaw, no premolars (Table 1.1).

