Menstrual cycle and its violations.
Dysfunctional uterine bleeding.
Questions:
1. Menstrual cycle.
2. Menstrual irregularities.
3. DUB - dysfunctional uterine bleeding.
Menstrual cycle.
Menstrual cycle is a rhythmically repeating biological process that prepares a woman’s body for pregnancy.
Menstruation- These are monthly, cyclically appearing uterine bleeding. The first menstruation (menarche) most often appears at 12-13 years of age (+/- 1.5-2 years). Menstruation most often stops at 45-50 years of age.
The menstrual cycle is conventionally defined from the first day of the previous to the first day of the next menstruation.
The physiological menstrual cycle is characterized by:
1. Two-phase.
2. Lasting no less than 22 and no more than 35 days (for 60% of women – 28-32 days). A menstrual cycle lasting less than 22 days is called anteponing, and more than 35 days is called postponing.
3. Constant cyclicality.
4. The duration of menstruation is 2-7 days.
5. Menstrual blood loss is 50-150 ml.
6. The absence of painful manifestations and disorders of the general condition of the body.
Regulation of the menstrual cycle.
There are 5 parts involved in the regulation of the menstrual cycle:
Cortex.
Hypothalamus.
Pituitary.
Ovaries.
I. Extrahypothalamic cerebral structures perceive impulses from the external environment and interoceptors and transmit them using neurotransmitters (a system of nerve impulse transmitters) to the neurosecretory nuclei of the hypothalamus.
Neurotransmitters include: dopamine, norepinephrine, serotonin, indole and new class morphine-like opioid neuropeptides - endorphins, enkephalins, donorphins.
II. The hypothalamus plays the role of a trigger mechanism. The nuclei of the hypothalamus produce pituitary hormones (releasing hormones) - liberins.
The pituitary luteinizing hormone releasing hormone (LHH, luliberin) was isolated, synthesized and described. RHLH and its synthetic analogues have the ability to stimulate the release of both LH and FSH by the pituitary gland. For hypothalamic gonadotropic liberins, a single name has been adopted: RHLH.
Releasing hormones enter the anterior lobe of the pituitary gland through a special vascular (portal) circulatory system.
Rice. Functional structure of the reproductive system.
Neurotransmitters (dopamine, norepinephrine, serotonin; opioid peptides;
β-endorphins enkephalin); Ok-oxytocin; P-progesterone; E-estrogens;
A-androgens; R-relaxin; I-inhibin.
III. The pituitary gland is the third level of regulation.
Pituitary comprises adenohypophysis (anterior lobe) and neurohypophysis (posterior lobe).
Adenohypophysis secretes tropic hormones:
§ Gonadotropic hormones:
¨ LH – luteinizing hormone
¨ FSH – follicle stimulating hormone
¨ PRL - prolactin
§ Tropic hormones
¨ STH – somatotropin
¨ ACTH – corticotropin
¨ TSH – thyrotropin.
Follicle-stimulating hormone stimulates the growth, development and maturation of the follicle in the ovary. With the help of luteinizing hormone, the follicle begins to function - to synthesize estrogens; without LH, ovulation and the formation of the corpus luteum do not occur. Prolactin, together with LH, stimulates the synthesis of progesterone by the corpus luteum, its main biological role– growth and development of the mammary glands and regulation of lactation. FSH peaks on the seventh day of the menstrual cycle and LH ovulatory peak on the fourteenth day.
IV. The ovary performs two functions:
1) generative (maturation of follicles and ovulation).
2) endocrine (synthesis steroid hormones– estrogens and progesterone).
At the birth of a girl, both ovaries contain up to 500 million primordial follicles. By the beginning of adolescence, due to atresia, their number is halved. During the entire reproductive period of a woman's life, only about 400 follicles mature.
The ovarian cycle consists of two phases:
Phase 1 – follicular
Phase 2 – luteal
Folliculin phase begins after the end of menstruation and ends with ovulation.
Luteal phase begins after ovulation and ends with the appearance of menstruation.
From the seventh day of the menstrual cycle, several follicles begin to grow simultaneously in the ovary. From the seventh day, one of the follicles is ahead of the others in development, by the time of ovulation it reaches a diameter of 20-28 mm, has a more pronounced capillary network and is called dominant. The dominant follicle contains an egg, its cavity is filled with follicular fluid. By the time of ovulation, the volume of follicular fluid increases 100 times, the content of estradiol (E 2) sharply increases in it, the rise in the level of which stimulates the release of LH by the pituitary gland. The follicle develops in the first phase of the menstrual cycle, which lasts until the 14th day, and then the mature follicle ruptures - ovulation.
During ovulation, follicular fluid pours out through the resulting hole and carries out the oocyte, surrounded by cells of the corona radiata. An unfertilized egg dies after 12-24 hours. After its release into the cavity of the follicle, the forming capillaries quickly grow, granulosa cells undergo luteinization - a corpus luteum is formed, the cells of which synthesize progesterone. In the absence of pregnancy, the corpus luteum transforms into a whitish body. The stage of functioning of the whitish body is 10-12 days, and then reverse development and regression occurs.
Granulosa cells of the follicle produce estrogens:
– Estrone (E 1 )
– Estradiol (E 2 )
– Estriol (E 3 )
The corpus luteum produces progesterone:
Progesterone prepares the endometrium and uterus for implantation of a fertilized egg and the development of pregnancy, and the mammary glands for lactation; suppresses the excitability of the myometrium. Progesterone has an anabolic effect and causes an increase in rectal temperature in the second phase of the menstrual cycle.
Androgens are synthesized in the ovary:
Androstenedione (precursor of testosterone) in the amount of 15 mg/day.
Dehydroepiandrosterone
Dehydroepiandrosterone sulfate
In the granulosa cells of the follicles, the protein hormone inhibin is formed, which inhibits the release of FSH by the pituitary gland, and local protein substances - oxytocin and relaxin. Oxytocin in the ovary promotes regression of the corpus luteum. The ovary also produces prostaglandins, which are involved in ovulation.
V. The uterus is the target organ for ovarian hormones.
There are 4 phases in the uterine cycle:
1. Desquamation phase
2.  Regeneration phase
Regeneration phase
3. Proliferation phase
4. Secretion phase
Phase proliferation begins with the regeneration of the functional layer of the endometrium and ends by the 14th day of the 28-day menstrual cycle with the full development of the endometrium. It is caused by the influence of FSH and ovarian estrogens.
Phase secretion lasts from the middle of the menstrual cycle until the beginning of the next menstruation. If pregnancy does not occur in a given menstrual cycle, the corpus luteum undergoes reverse development, which leads to a drop in the level of estrogen and progesterone. Hemorrhages occur in the endometrium; its necrosis and rejection of the functional layer occur, i.e. menstruation begins ( desquamation phase ).
Cyclic processes under the influence of sex hormones also occur in other target organs, which include the tubes, vagina, external genitalia, mammary glands, hair follicles, skin, bones, and adipose tissue. The cells of these organs and tissues contain receptors for sex hormones.
Menstrual irregularities:
Disorders of menstrual function occur when its regulation is disrupted at various levels and can be due to the following reasons:
Diseases and disorders of the nervous and endocrine system
1. pathology of puberty
2. mental and nervous diseases
3. emotional turmoil
Poor nutrition
Occupational hazards
Infectious and somatic diseases
Amenorrhea- is the absence of menstruation for 6 months or more in women 16-45 years old.

Physiological amenorrhea:
– during pregnancy
– during lactation
– before puberty
– postmenopausal
Pathological amenorrhea is a symptom of many genital and extragenital diseases.
– True amenorrhea, in which there is no menstruation and cyclical processes in the body
– False amenorrhea (cryptomenorrhea) – absence of external manifestations, i.e. menstrual bleeding (in the presence of cyclical processes in the body): this happens with atresia of the hymen, cervical canal, vagina and other malformations of the female reproductive system.
True amenorrhea (primary and secondary)
Primary amenorrhea: is the absence of menstruation in a girl aged 16 years or older (who has never had menstruation).
æPrimary amenorrhea
1. hypogonadotropic amenorrhea.
Clinic:
Patients have eunuchoid body features
Hypoplasia of the mammary glands with fat replacement glandular tissue
The size of the uterus and ovaries corresponds to the age of 2-7 years
Treatment: hormone therapy with gonadotropic hormones and cyclic therapy with combined oral contraceptives 3-4 months.
2. Primary amenorrhea against the background of virilization symptoms – This congenital adrenogenital syndrome (CAS). In this syndrome, there are genetically determined disorders of androgen synthesis in the adrenal cortex.
3. Primary amenorrhea with a normal phenotype can be caused by malformations of the uterus, vagina - testicular feminization syndrome.
Testicular feminization syndrome is a rare pathology (1 case in 12,000-15,000 newborns). It is one of the monogenic mutations - a change in one gene leads to the congenital absence of the enzyme 5α-reductase, which converts testosterone into more active dehydrotestosterone.
§ Karyotype in patients – 46 xy.
§ At birth, the female type of structure of the external genitalia is noted
§ The vagina is short, blind
§ The gonads in 1/3 of patients are located in the abdominal cavity, in 1/3 – in the inguinal canals, and in the rest – in the thickness of the labia. Sometimes there is a congenital inguinal hernia that contains the testicle.
§ The phenotype of adult patients is female.
§ The mammary glands are well developed. The nipples are underdeveloped, the parapapillary areas are weakly expressed. Genital and axillary hair growth was not detected.
Treatment: surgical (removal of defective testicles) at the age of 16-18 years after completion of growth and development of secondary sexual characteristics.
4. Gonadal dysgenesis (genetically determined ovarian malformation)
Due to the quantitative and qualitative defect of sex chromosomes, normal development of ovarian tissue does not occur and connective tissue cords are formed in place of the ovaries, and this causes a sharp deficiency of sex hormones.
Gonadal dysgenesis has 3 clinical forms:
1) Shereshevsky-Turner syndrome
2) “Pure” form of gonadal dysgenesis
3) Mixed form of gonadal dysgenesis
The menstrual cycle is cyclically repeating changes in a woman’s body, especially in the parts of the reproductive system, the external manifestation of which is blood discharge from the genital tract - menstruation.
The menstrual cycle is established after menarche (first menstruation) and continues throughout the reproductive, or childbearing, period of a woman’s life with the ability to reproduce. Cyclic changes in a woman’s body are two-phase. The first (follicular) phase of the cycle is determined by the maturation of the follicle and egg in the ovary, after which it ruptures and the egg is released from it - ovulation. The second (luteal) phase is associated with the formation of the corpus luteum. At the same time, in a cyclic mode, regeneration and proliferation of the functional layer successively occur in the endometrium, followed by the secretory activity of its glands. Changes in the endometrium result in desquamation of the functional layer (menstruation).
The biological significance of the changes that occur during the menstrual cycle in the ovaries and endometrium is to ensure reproductive function at the stages of egg maturation, its fertilization and implantation of the embryo in the uterus. If fertilization of the egg does not occur, the functional layer of the endometrium is rejected, and bloody issues, and in the reproductive system again, and in the same sequence, processes occur aimed at ensuring the maturation of the egg.
Menstruation is bloody discharge from the genital tract that repeats at certain intervals throughout the reproductive period of a woman’s life outside of pregnancy and lactation. Menstruation is the culmination of the menstrual cycle and occurs at the end of its luteal phase as a result of the rejection of the functional layer of the endometrium. The first menstruation (menarhe) occurs at the age of 10–12 years. Over the next 1–1.5 years, menstruation may be irregular, and only then a regular menstrual cycle is established.
The first day of menstruation is conventionally taken as the first day of the cycle, and the duration of the cycle is calculated as the interval between the first days of the two subsequent menstruation.
1. duration from 21 to 35 days (for 60% of women, the average cycle length is 28 days);
2. duration of menstrual flow from 2 to 7 days;
3. the amount of blood loss on menstrual days is 40–60 ml (on average 50 ml).
In neuroendocrine regulation, 5 levels can be distinguished, interacting according to the principle of direct and inverse positive and negative relationships.
The first (highest) level of regulation of the functioning of the reproductive system is the structures that make up the acceptor of all external and internal (from the subordinate departments) influences - the cerebral cortex of the central nervous system and extrahypothalamic cerebral structures (limbic system, hippocampus, amygdala).
It is well known about the possibility of stopping menstruation under severe stress (loss of loved ones, wartime conditions, etc.), as well as without obvious external influences due to general mental imbalance (“false pregnancy” - delayed menstruation due to strong desire or if you have a strong fear of getting pregnant).
Internal influences are perceived through specific receptors for the main sex hormones: estrogens, progesterone and androgens.
In response to external and internal stimuli in the cerebral cortex and extrahypothalamic structures, the synthesis, release and metabolism of neuropeptides, neurotransmitters occur, as well as the formation of specific receptors, which, in turn, selectively influence the synthesis and release of the hypothalamic releasing hormone.
The most important neurotransmitters, i.e. transmitter substances, include norepinephrine, dopamine, gamma-aminobutyric acid (GABA), acetylcholine, serotonin and melatonin.
Cerebral neurotransmitters regulate the production of gonadotropin-releasing hormone (GnRH): norepinephrine, acetylcholine and GABA stimulate their release, while dopamine and serotonin have the opposite effect.
Neuropeptides (endogenous opioid peptides - EOP, corticotropin-releasing factor and galanin) also affect the function of the hypothalamus and the balanced functioning of all parts of the reproductive system.
Currently, there are 3 groups of EOPs: enkephalins, endorphins and dynorphins. According to modern concepts, EOPs are involved in the regulation of GnRH formation. An increase in the level of EOP suppresses the secretion of GnRH, and, consequently, the release of LH and FSH, which may be the cause of anovulation, and in more severe cases, amenorrhea. The administration of opioid receptor inhibitors (drugs such as naloxone) normalizes the formation of GnRH, which helps normalize ovulatory function and other processes in the reproductive system in patients with central amenorrhea.
When the level of sex steroids decreases (with age-related or surgical shutdown of ovarian function), EOPs do not have an inhibitory effect on the release of GnRH, which likely causes increased production of gonadotropins in postmenopausal women.
Thus, the balance of the synthesis and subsequent metabolic transformations of neurotransmitters, neuropeptides and neuromodulators in the neurons of the brain and in the suprahypothalamic structures ensures the normal course of processes associated with ovulatory and menstrual function.
The second level of regulation of reproductive function is the hypothalamus, in particular, its hypophysiotropic zone, consisting of neurons of the ventro- and dorsomedial arcuate nuclei, which have neurosecretory activity. These cells have the properties of both neurons (reproducing regulatory electrical impulses) and endocrine cells, which have either a stimulating (liberins) or blocking (statins) effect. The activity of neurosecretion in the hypothalamus is regulated both by sex hormones that come from the bloodstream and by neurotransmitters and neuropeptides produced in the cerebral cortex and suprahypothalamic structures.
The hypothalamus secretes GnRH, which contains follicle-stimulating hormones (RGFSH - folliberin) and luteinizing hormones (RGLH - luliberin) that act on the pituitary gland.
The decapeptide RHLH and its synthetic analogues stimulate the release of not only LH, but also FSH by gonadotrophs. In this regard, one term has been adopted for gonadotropic liberins - gonadotropin-releasing hormone (GnRH).
The synthesis of hypothalamic liberin, which stimulates the formation of prolactin, is activated by TSH-releasing hormone (thyrotropin-releasing hormone). The formation of prolactin is also activated by serotonin and endogenous opioid peptides that stimulate the serotonergic systems. Dopamine, on the contrary, inhibits the release of prolactin from lactotrophs of the adenohypophysis. The use of dopaminergic drugs such as parlodel (bromocriptine) can successfully treat functional and organic hyperprolactinemia, which is a very common cause of menstrual and ovulatory dysfunction.
The secretion of GnRH is genetically programmed and has a pulsatile (circhoral) nature, peaks of enhanced hormone secretion lasting several minutes are replaced by 1-3 hour intervals of relatively low secretory activity. The frequency and amplitude of GnRH secretion is regulated by the level of estradiol - GnRH emissions in the preovulatory period against the background of maximum estradiol secretion are significantly greater than in the early follicular and luteal phases.
The third level of regulation of reproductive function is the anterior lobe of the pituitary gland, which secretes gonadotropic hormones - follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin, adrenocorticotropic hormone (ACTH), somatotropic hormone (GH) and thyroid-stimulating hormone(TSG). Normal functioning of the reproductive system is possible only with a balanced selection of each of them.
FSH stimulates the growth and maturation of follicles and proliferation of granulosa cells in the ovary; formation of FSH and LH receptors on granulosa cells; aromatase activity in the ripening follicle (this enhances the conversion of androgens to estrogens); production of inhibin, activin and insulin-like growth factors.
LH promotes the formation of androgens in theca cells; ovulation (together with FSH); remodeling of granulosa cells during luteinization; synthesis of progesterone in the corpus luteum.
Prolactin has a variety of effects on a woman’s body. Its main biological role is stimulation of mammary gland growth, regulation of lactation, as well as control of progesterone secretion by the corpus luteum by activating the formation of LH receptors in it. During pregnancy and lactation, inhibition of prolactin synthesis and, as a consequence, an increase in its level in the blood stops.
The fourth level of regulation of reproductive function includes peripheral endocrine organs (ovaries, adrenal glands, thyroid). The main role belongs to the ovaries, and other glands perform their own specific functions, while simultaneously maintaining the normal functioning of the reproductive system.
The growth and maturation of follicles, ovulation, the formation of the corpus luteum, and the synthesis of sex steroids occur in the ovaries.
At birth, a girl’s ovaries contain approximately 2 million primordial follicles. By the time of menarche, the ovaries contain 200–400 thousand primordial follicles. During one menstrual cycle, as a rule, only one follicle with an egg inside develops. If a larger number matures, a multiple pregnancy is possible.
Folliculogenesis begins under the influence of FSH in the late part of the luteal phase of the cycle and ends at the beginning of the peak of gonadotropin secretion. Approximately 1 day before the onset of menstruation, the level of FSH increases again, which ensures the entry into growth, or recruitment, of follicles (1–4 days of the cycle), selection of follicles from a cohort of homogeneous - quasi-synchronized (5–7 days), maturation dominant follicle(days 8–12) and ovulation (days 13–15). As a result, a preovulatory follicle is formed, and the rest of the cohort of follicles that have entered into growth undergo atresia.
Depending on the stage of development and morphological characteristics, primordial, preantral, antral and preovulatory, or dominant, follicles are distinguished.
The primordial follicle consists of an immature egg, which is located in the follicular and granulosa (granular) epithelium. Outside, the follicle is surrounded by a connective tissue membrane (theca cells). During each menstrual cycle, 3 to 30 primordial follicles begin to grow, becoming preantral (primary) follicles.
Preantral follicle. In the preantral follicle, the oocyte increases in size and is surrounded by a membrane called the zona pellucida. Granulosa epithelial cells proliferate and round to form the stratum granulosum, and the theca layer is formed from the surrounding stroma.
The preovulatory (dominant) follicle stands out among the growing follicles the most large size(diameter at the time of ovulation reaches 20 mm). The dominant follicle has a richly vascularized layer of theca cells and granulosa cells with a large number of receptors for FSH and LH. Along with the growth and development of the dominant preovulatory follicle in the ovaries, atresia of the remaining initially growing (recruited) follicles occurs in parallel, and atresia of the primordial follicles also continues.
During maturation, a 100-fold increase in the volume of follicular fluid occurs in the preovulatory follicle. During the maturation of antral follicles, the composition of the follicular fluid changes.
The antral (secondary) follicle undergoes an enlargement of the cavity formed by the accumulating follicular fluid produced by the cells of the granulosa layer. The activity of sex steroid formation also increases. Androgens (androstenedione and testosterone) are synthesized in the theca cells. Once in granulosa cells, androgens actively undergo aromatization, which causes their conversion into estrogens.
At all stages of follicle development, except preovulatory, the progesterone content is at a constant and relatively low level. There are always fewer gonadotropins and prolactin in follicular fluid than in blood plasma, and the level of prolactin tends to decrease as the follicle matures. FSH is detected from the beginning of cavity formation, and LH can only be detected in the mature preovulatory follicle along with progesterone. Follicular fluid also contains oxytocin and vasopressin, and in concentrations 30 times higher than in the blood, which may indicate local formation of these neuropeptides. Prostaglandins of classes E and F are detected only in the preovulatory follicle and only after the start of the rise in LH levels, which indicates their targeted involvement in the ovulation process.
Ovulation is the rupture of the preovulatory (dominant) follicle and the release of an egg. Ovulation is accompanied by bleeding from the destroyed capillaries surrounding theca cells. It is believed that ovulation occurs 24–36 hours after the preovulatory peak of estradiol, causing a sharp rise in LH secretion. Against this background, proteolytic enzymes - collagenase and plasmin - are activated, destroying the collagen of the follicle wall and thus reducing its strength. At the same time, the observed increase in the concentration of prostaglandin F2a, as well as oxytocin, induces rupture of the follicle as a result of their stimulation of smooth muscle contraction and expulsion of the oocyte with the egg-bearing mound from the follicle cavity. The rupture of the follicle is also facilitated by an increase in the concentration of prostaglandin E2 and relaxin in it, which reduce the rigidity of its walls.
After the release of the egg into the cavity of the ovulated follicle, the resulting capillaries quickly grow. Eranulosa cells undergo luteinization, which is morphologically manifested in an increase in their Volume and the formation of lipid inclusions. This process, leading to the formation of the corpus luteum, is stimulated by LH, which actively interacts with specific receptors of granulosa cells.
The corpus luteum is a transient hormonally active formation that functions for 14 days, regardless of the total duration of the menstrual cycle. If pregnancy does not occur, the corpus luteum regresses. A full-fledged corpus luteum develops only in the phase when an adequate number of granulosa cells with a high content of LH receptors are formed in the preovulatory follicle.
In addition to steroid hormones and inhibins that enter the bloodstream and affect target organs, biologically active compounds with a predominantly local hormone-like effect are synthesized in the ovaries. Thus, the formed prostaglandins, oxytocin and vasopressin play an important role as ovulation triggers. Oxytocin also has a luteolytic effect, ensuring regression of the corpus luteum. Relaxin promotes ovulation and has a tocolytic effect on the myometrium. Growth factors - epidermal growth factor (EGF) and insulin-like growth factors 1 and 2 (IGF-1 and IGF-2) activate the proliferation of granulosa cells and the maturation of follicles. These same factors participate, together with gonadotropins, in the fine regulation of the processes of selection of the dominant follicle, atresia of degenerating follicles of all stages, as well as in the cessation of the functioning of the corpus luteum.
The phenomenon of the “menstrual wave” in the days preceding menstruation is associated with receptors for sex steroids in the central nervous system, in the structures of the hippocampus that regulate the emotional sphere, as well as in the centers that control autonomic functions. This phenomenon is manifested by an imbalance in the processes of activation and inhibition in the cortex, fluctuations in the tone of the sympathetic and parasympathetic systems (especially noticeably affecting the functioning of the cardiovascular system), as well as changes in mood and some irritability. In healthy women, these changes, however, do not go beyond physiological limits.
The fifth level of regulation of reproductive function consists of the internal and external parts of the reproductive system (uterus, fallopian tubes, vaginal mucosa), sensitive to fluctuations in the levels of sex steroids, as well as the mammary glands. The most pronounced cyclic changes occur in the endometrium.
Cyclic changes in the endometrium concern its surface layer, consisting of compact epithelial cells, and the intermediate layer, which are rejected during menstruation.
The basal layer, which is not rejected during menstruation, ensures the restoration of desquamated layers.
Based on changes in the endometrium during the cycle, the proliferation phase, the secretion phase and the bleeding phase (menstruation) are distinguished.
The proliferation phase (follicular) lasts an average of 12–14 days, starting from the 5th day of the cycle. During this period, a new surface layer is formed with elongated tubular glands lined with columnar epithelium with increased mitotic activity. The thickness of the functional layer of the endometrium is 8 mm.
The secretion phase (luteal) is associated with the activity of the corpus luteum and lasts 14 days (±1 day). During this period, the epithelium of the endometrial glands begins to produce secretions containing acidic glycosaminoglycans, glycoproteins, and glycogen.
Secretion activity becomes highest on days 20–21. By this time, the maximum amount of proteolytic enzymes is found in the endometrium, and decidual transformations occur in the stroma. There is a sharp vascularization of the stroma - the spiral arteries are sharply tortuous, forming “tangles” found throughout the entire functional layer. The veins are dilated. Such changes in the endometrium, observed on days 20–22 (days 6–8 after ovulation) of the 28-day menstrual cycle, provide the best conditions for implantation of a fertilized egg.
By the 24th–27th day, due to the beginning of regression of the corpus luteum and a decrease in the concentration of hormones produced by it, the trophism of the endometrium is disrupted with a gradual increase in degenerative changes in it. In the superficial areas of the compact layer, lacunar expansion of capillaries and hemorrhages into the stroma are noted, which can be detected within 1 day. before the start of menstruation.
Menstruation involves desquamation and regeneration of the functional layer of the endometrium. The onset of menstruation is facilitated by prolonged spasm of the arteries, leading to blood stasis and the formation of blood clots. Lysosomal proteolytic enzymes released from leukocytes enhance the melting of tissue elements. Following a prolonged spasm of blood vessels, their paretic dilation occurs with increased blood flow. At the same time, there is an increase in hydrostatic pressure in the microvasculature and rupture of the walls of blood vessels, which by this time have largely lost their mechanical strength. Against this background, active desquamation of necrotic areas of the functional layer occurs. By the end of the 1st day of menstruation, 2/3 of the functional layer is rejected, and its complete desquamation usually ends on the 3rd day.
Regeneration of the endometrium begins immediately after the rejection of the necrotic functional layer. Under physiological conditions, already on the 4th day of the cycle, the entire wound surface of the mucous membrane is epithelialized.
It has been established that the induction of the formation of receptors for both estradiol and progesterone depends on the concentration of estradiol in tissues.
The regulation of local concentrations of estradiol and progesterone is mediated to a large extent by the appearance of various enzymes during the menstrual cycle. The content of estrogens in the endometrium depends not only on their level in the blood, but also on their formation. A woman's endometrium is capable of synthesizing estrogens by converting androstenedione and testosterone with the participation of aromatase (aromatization).
IN Lately It has been established that the endometrium is capable of secreting prolactin, which is completely identical to that of the pituitary gland. Prolactin synthesis by the endometrium begins in the second half of the luteal phase (activated by progesterone) and coincides with the decidualization of stromal cells.
The cyclical activity of the reproductive system is determined by the principles of direct and feedback, which is provided by specific receptors for hormones in each of the links. The direct connection is the stimulating effect of the hypothalamus on the pituitary gland and the subsequent formation of sex steroids in the ovary. The feedback is determined by the effect of increased concentrations of sex steroids on higher levels.
In the interaction of parts of the reproductive system, “long”, “short” and “ultra-short” loops are distinguished. The “long” loop is the effect through the receptors of the hypothalamic-pituitary system on the production of sex hormones. The “short” loop defines the connection between the pituitary gland and the hypothalamus. "Ultrashort" loop - connection between the hypothalamus and nerve cells, which carry out local regulation using neurotransmitters, neuropeptides, neuromodulators and electrical stimuli.
| |
In the body of a sexually mature, non-pregnant woman, regularly repeating complex changes occur that prepare the body for pregnancy. These biologically important rhythmically repeating changes are called the menstrual cycle.
The length of the menstrual cycle varies. For most women, the cycle lasts 28-30 days, sometimes it is shortened to 21 days, and occasionally there are women who have a 35-day cycle. It must be remembered that menstruation does not mean the beginning, but the end of physiological processes; menstruation indicates the attenuation of processes that prepare the body for pregnancy, the death of an unfertilized egg. At the same time, menstrual bleeding is the most striking, noticeable manifestation of cyclic processes, so it is practically convenient to begin calculating the cycle from the first day of the last menstruation.
Rhythmically repeating changes during the menstrual cycle occur throughout the body. Many women experience irritability, fatigue and drowsiness before menstruation, followed by a feeling of vigor and energy after menstruation. Before menstruation, an increase in tendon reflexes, sweating, a slight increase in heart rate, an increase in blood pressure, and an increase in body temperature by several tenths of a degree are also observed. During menstruation, the pulse slows down somewhat, blood pressure and temperature drop slightly. After menstruation, all these phenomena disappear. Noticeable cyclic changes occur in the mammary glands. In the premenstrual period, there is a slight increase in their volume, tension, and sometimes sensitivity. After menstruation, these phenomena disappear. During a normal menstrual cycle, changes in the nervous system occur within the limits of physiological fluctuations and do not reduce women’s ability to work.
Reaction of the menstrual cycle. In the regulation of the menstrual cycle, five links can be distinguished: cerebral cortex, hypothalamus, pituitary gland, ovaries, uterus. The cerebral cortex sends nerve impulses to the hypothalamus. The hypothalamus produces neurohormones that were called releasing factors or liberins. They in turn have an effect on the pituitary gland. The pituitary gland has two lobes: anterior and posterior. The posterior lobe accumulates the hormones oxytocin and vasopressin, which are synthesized in the hypothalamus. A number of hormones are produced in the anterior lobe of the pituitary gland, including hormones that activate the activity of the ovaries. Hormones of the anterior pituitary gland that stimulate the functions of the ovary are called gonadotropins (gonadotropins).
The pituitary gland produces three hormones that act on the ovary: 1) follicle-stimulating hormone (FSH); it stimulates the growth and maturation of follicles in the ovary, as well as the formation of follicular (estrogenic) hormone;
2) luteinizing hormone (LH), which causes the development of the corpus luteum and the formation of the hormone progesterone in it;
3) lactogenic (luteotropic) hormone - prolactin, promotes the production of progesterone in combination with LH.
In addition to FSH, LTG, LH gonadotropins, TSH is produced in the anterior lobe of the pituitary gland, which stimulates the thyroid gland; HGH is a growth hormone; if it is deficient, dwarfism develops; if too much, gigantism develops; ACTH stimulates the adrenal glands.
There are two types of secretion of gonadotropic hormones: tonic (constant release at a low level) and cyclic (increased during certain phases of the menstrual cycle). An increase in FSH secretion is observed at the beginning of the cycle and especially in the middle of the cycle, around the time of ovulation. An increase in LH secretion is observed immediately before ovulation and during the development of the corpus luteum.
Ovarian cycle . Gonadotropic hormones are perceived by receptors (protein nature) of the ovary. Under their influence, rhythmically repeating changes occur in the ovary, which go through three phases:
a) follicle development - follicular phase, under the influence of FSH of the pituitary gland, from the 1st to the 14th – 15th day of the menstrual cycle with a 28-day menstrual cycle;
b) rupture of a mature follicle - ovulation phase, under the influence of FSH and LH of the pituitary gland on the 14th – 15th day of the menstrual cycle; During the ovulation phase, a mature egg is released from a ruptured follicle.
c) development of the corpus luteum - luteal phase, under the influence of LTG and LH of the pituitary gland from the 15th to 28th day of the menstrual cycle;
In the ovary in the follicular phase Estrogenic hormones are produced, they contain several fractions: estradiol, estrone, estriol. Estradiol is the most active; it mainly affects the changes inherent in the menstrual cycle.
During the luteal phase(development of the corpus luteum), a new, very important gland is formed in place of the ruptured follicle internal secretion- corpus luteum (corpus luteum), producing the hormone progesterone. The process of progressive development of the corpus luteum occurs during a 28-day cycle over 14 days and occupies the second half of the cycle - from ovulation to the next menstruation. If pregnancy does not occur, then from the 28th day of the cycle the reverse development of the corpus luteum begins. In this case, the death of luteal cells, emptying of blood vessels and proliferation of connective tissue occur. As a result, a scar forms in place of the corpus luteum - white body, which subsequently also disappears. The corpus luteum is formed with each menstrual cycle; if pregnancy does not occur, it is called the corpus luteum of menstruation.
Uterine cycle. Under the influence of ovarian hormones formed in the follicle and corpus luteum, cyclic changes in the tone, excitability and blood supply of the uterus occur. However, the most significant cyclic changes are observed in the functional layer of the endometrium. The uterine cycle, like the ovarian cycle, lasts 28 days (less often 21 or 30-35 days). It distinguishes the following phases: a) desquamation;
b) regeneration; c) proliferation; d) secretion.
Desquamation phase manifested by menstrual bleeding, usually lasting 3-7 days; This is actually menstruation. The functional layer of the mucous membrane disintegrates, is rejected and is released out along with the contents of the uterine glands and blood from the opened vessels. The phase of endometrial desquamation coincides with the beginning of the death of the corpus luteum in the ovary.
Regeneration phase(restoration) of the mucous membrane begins during the period of desquamation and ends by the 5th - 7th day from the beginning of menstruation. Restoration of the functional layer of the mucous membrane occurs due to the proliferation of the epithelium of the remnants of the glands located in the basal layer and the proliferation of other elements of this layer (stroma, vessels, nerves).
Proliferation phase endometrium coincides with the maturation of the follicle in the ovary and continues until the 14th day of the cycle (with a 21-day cycle until the 10-11th day). Under the influence of estrogen (follicular) hormone proliferation (growth) of the stroma and growth of the glands of the endometrial mucosa occur. The glands stretch out in length, then twist like a corkscrew, but do not contain a secretion. The vascular network grows, the number of spiral arteries increases. The mucous membrane of the uterus thickens 4-5 times during this period.
Secretion phase coincides with the development and flowering of the corpus luteum in the ovary and lasts from the 14-15th day to the 28th, i.e. until the end of the cycle.
Under the influence of progesterone Important qualitative transformations occur in the uterine mucosa. The glands begin to produce secretions, their cavity expands. Glycoproteins, glycogen, phosphorus, calcium, trace elements and other substances are deposited in the mucous membrane. As a result of these changes in the mucous membrane, conditions are created that are favorable for the development of the embryo. If pregnancy does not occur, the corpus luteum dies, the functional layer of the endometrium, which has reached the secretion phase, is rejected, and menstruation occurs.
These cyclic changes are repeated at regular intervals during a woman's puberty. The cessation of cyclic processes occurs due to such physiological processes like pregnancy and breastfeeding. Disruption of menstrual cycles is also observed under pathological conditions (severe illnesses, mental influences, malnutrition, etc.).
LECTURE: SEX HORMONES OF WOMEN AND MEN, THEIR BIOLOGICAL ROLE.
Sex hormones are produced in the ovaries - estrogens, androgens, produced by the cells of the inner lining of the follicle, progesterone-yellow body. Estrogens are distinguished between more active ones (estradiol and estrone, or folliculin) and less active ones (estriol). In terms of their chemical structure, estrogens are close to the hormones of the corpus luteum, adrenal cortex and male sex hormones. All of them are based on a steroid ring and differ only in the structure of the side chains.
ESTROGEN HORMONES.
Estrogens are classified as steroid hormones. The ovaries produce 17 mg of estrogen-estradiol per day. Largest quantity it is secreted in the middle of the menstrual cycle (on the eve of ovulation), the least - at the beginning and at the end. Before menstruation, the amount of estrogen in the blood decreases sharply.
In total, the ovaries produce about 10 mg of estrogen during the cycle.
The effect of estrogen on a woman’s body:
- During puberty, estrogen hormones cause the growth and development of the uterus, vagina, external genitalia, as well as the appearance of secondary sexual characteristics.
- During puberty, estrogenic hormones cause regeneration and proliferation of cells in the uterine mucosa.
3. Estrogens increase the tone of the muscles of the uterus, increase its excitability and sensitivity to substances that contract the uterus.
4. During pregnancy, estrogen hormones ensure the growth of the uterus and the restructuring of its neuromuscular system.
5. Estrogens cause the onset of labor.
6. Estrogens promote the development and function of the mammary glands.
Starting from the 13-14th week of pregnancy, the placenta takes over the estrogenic function. With insufficient production of estrogen, primary weakness of labor is observed, which negatively affects the condition of the mother and especially the intrauterine fetus, as well as the newborn. They affect the level and metabolism of calcium in the uterus, as well as water metabolism, which is expressed by cyclic fluctuations in a woman’s weight associated with changes in water content in the body during the menstrual cycle. With the introduction of small and medium doses of estrogens, the body's resistance to infections increases.
Currently, the industry produces the following estrogen drugs: estradiol propionate, estradiol benzoate, estrone (folliculin), estriol (sinestrol), diethylstilbestrol, diethylstilbestrol propionate, dienestrol acetate, dimestrol, acrofollin, hogival, ethinylestradiol, microfollin, etc.
Substances that can neutralize and block the specific effects of estrogen drugs are called antiestrogens. These include androgens and gestagens.
Chapter 2. NEUROENDOCRINE REGULATION OF THE MENSTRUAL CYCLE
Menstrual cycle - genetically determined, cyclically repeating changes in a woman’s body, especially in parts of the reproductive system, the clinical manifestation of which is blood discharge from the genital tract (menstruation).
The menstrual cycle is established after menarche (first menstruation) and continues throughout the reproductive (childbearing) period of a woman's life until menopause (last menstruation). Cyclic changes in a woman’s body are aimed at the possibility of reproducing offspring and are of a two-phase nature: the 1st (follicular) phase of the cycle is determined by the growth and maturation of the follicle and egg in the ovary, after which the follicle ruptures and the egg leaves it - ovulation; The 2nd (luteal) phase is associated with the formation of the corpus luteum. At the same time, successive changes in the endometrium occur in a cyclic mode: regeneration and proliferation of the functional layer, followed by secretory transformation of the glands. Changes in the endometrium result in desquamation of the functional layer (menstruation).
The biological significance of the changes that occur during the menstrual cycle in the ovaries and endometrium is to ensure reproductive function after the maturation of the egg, its fertilization and implantation of the embryo in the uterus. If fertilization of the egg does not occur, the functional layer of the endometrium is rejected, blood discharge appears from the genital tract, and processes aimed at ensuring the maturation of the egg occur in the reproductive system again and in the same sequence.
Menstruation - This is bleeding from the genital tract that is repeated at certain intervals throughout the entire reproductive period, excluding pregnancy and lactation. Menstruation begins at the end of the luteal phase of the menstrual cycle as a result of the rejection of the functional layer of the endometrium. First menstruation (menarhe) occurs at the age of 10-12 years. Over the next 1-1.5 years, menstruation may be irregular, and only then a regular menstrual cycle is established.
The first day of menstruation is conventionally taken as the 1st day of the menstrual cycle, and the duration of the cycle is calculated as the interval between the first days of two consecutive menstruation periods.
External parameters of a normal menstrual cycle:
Duration - from 21 to 35 days (in 60% of women, the average cycle length is 28 days);
The duration of menstrual flow is from 3 to 7 days;
The amount of blood loss on menstrual days is 40-60 ml (on average
The processes that ensure the normal course of the menstrual cycle are regulated by a single functionally related neuroendocrine system, including central (integrating) sections, peripheral (effector) structures, as well as intermediate links.
The functioning of the reproductive system is ensured by a strictly genetically programmed interaction of five main levels, each of which is regulated by overlying structures according to the principle of direct and inverse, positive and negative relationships (Fig. 2.1).
The first (highest) level of regulation reproductive system are cortex And extrahypothalamic cerebral structures
(limbic system, hippocampus, amygdala). An adequate state of the central nervous system ensures the normal functioning of all underlying parts of the reproductive system. Various organic and functional changes in the cortex and subcortical structures can lead to menstrual irregularities. The possibility of stopping menstruation under severe stress (loss of loved ones, wartime conditions, etc.) or without obvious external influences due to general mental imbalance ("false pregnancy" - delayed menstruation with a strong desire for pregnancy or, conversely, with fear of it) is well known ).
Specific neurons of the brain receive information about the state of both the external and internal environment. The internal effect is carried out using specific receptors for ovarian steroid hormones (estrogens, progesterone, androgens) located in the central nervous system. In response to the influence of environmental factors on the cerebral cortex and extrahypothalamic structures, synthesis, excretion and metabolism occur neurotransmitters And neuropeptides. In turn, neurotransmitters and neuropeptides influence the synthesis and release of hormones by the neurosecretory nuclei of the hypothalamus.
To the most important neurotransmitters, those. substances that transmit nerve impulses include norepinephrine, dopamine, γ-aminobutyric acid (GABA), acetylcholine, serotonin and melatonin. Norepinephrine, acetylcholine and GABA stimulate the release of gonadotropin releasing hormone (GnRH) by the hypothalamus. Dopamine and serotonin reduce the frequency and amplitude of GnRH production during the menstrual cycle.
Neuropeptides(endogenous opioid peptides, neuropeptide Y, galanin) are also involved in the regulation of the function of the reproductive system. Opioid peptides (endorphins, enkephalins, dynorphins), binding to opiate receptors, lead to suppression of GnRH synthesis in the hypothalamus.
Rice. 2.1. Hormonal regulation in the system hypothalamus - pituitary gland - peripheral endocrine glands - target organs (diagram): RG - releasing hormones; TSH - thyroid-stimulating hormone; ACTH - adrenocoticotropic hormone; FSH - follicle-stimulating hormone; LH - luteinizing hormone; Prl - prolactin; P - progesterone; E - estrogens; A - androgens; R - relaxin; I - ingi-bin; T 4 - thyroxine, ADH - antidiuretic hormone (vasopressin)
Second level regulation of reproductive function is hypothalamus. Despite its small size, the hypothalamus is involved in the regulation of sexual behavior, controls vegetative-vascular reactions, body temperature and other vital functions. important functions body.
Pituitary zone of the hypothalamus represented by groups of neurons that make up the neurosecretory nuclei: ventromedial, dorsomedial, arcuate, supraoptic, paraventricular. These cells have the properties of both neurons (reproducing electrical impulses) and endocrine cells that produce specific neurosecrets with diametrically opposed effects (liberins and statins). Li-beryns, or releasing factors, stimulate the release of corresponding tropic hormones in the anterior pituitary gland. Statins have an inhibitory effect on their secretion. Currently, seven liberins are known, which are decapeptides in nature: thyreoliberin, corticoliberin, somatoliberin, melanoliberin, folliberin, luliberin, prolactoliberin, as well as three statins: melanostatin, somatostatin, prolactostatin, or prolactin-inhibiting factor.
Luliberin, or luteinizing hormone releasing hormone (LHR), has been isolated, synthesized and described in detail. To date, it has not been possible to isolate and synthesize follicle-stimulating releasing hormone. However, it has been established that RHLH and its synthetic analogues stimulate the release of not only LH by gonadotrophs, but also FSH. In this regard, one term has been adopted for gonadotropic liberins - “gonadotropin-releasing hormone” (GnRH), which is essentially a synonym for luliberin (RLH).
The main site of GnRH secretion is the arcuate, supraoptic and paraventricular nuclei of the hypothalamus. The arcuate nuclei reproduce a secretory signal with a frequency of approximately 1 impulse per 1-3 hours, i.e. V pulsating or circhoral mode (circhoral- around an hour). These impulses have a certain amplitude and cause periodic flow of GnRH through the portal blood flow system to the cells of the adenohypophysis. Depending on the frequency and amplitude of GnRH pulses, preferential secretion of LH or FSH occurs in the adenohypophysis, which, in turn, causes morphological and secretory changes in the ovaries.
The hypothalamic-pituitary region has a special vascular network called portal system. A feature of this vascular network is the ability to transmit information both from the hypothalamus to the pituitary gland and vice versa (from the pituitary gland to the hypothalamus).
Regulation of prolactin release is largely under the influence of statin. Dopamine, produced in the hypothalamus, inhibits the release of prolactin from the lactotrophs of the adenohypophysis. Thyroliberin, as well as serotonin and endogenous opioid peptides, contribute to an increase in the secretion of prolactin.
In addition to liberins and statins, two hormones are produced in the hypothalamus (supraoptic and paraventricular nuclei): oxytocin and vasopressin (antidiuretic hormone). Granules containing these hormones migrate from the hypothalamus along the axons of magnocellular neurons and accumulate in the posterior lobe of the pituitary gland (neurohypophysis).
Third level The pituitary gland regulates reproductive function; it consists of an anterior, posterior and intermediate (middle) lobe. Directly related to the regulation of reproductive function is anterior lobe (adenohypophysis) . Under the influence of the hypothalamus, gonadotropic hormones are secreted in the adenohypophysis - FSH (or follitropin), LH (or lutropin), prolactin (Prl), ACTH, somatotropic (STH) and thyroid-stimulating (TSH) hormones. Normal functioning of the reproductive system is possible only with a balanced selection of each of them.
Gonadotropic hormones (FSH, LH) of the anterior pituitary gland are under the control of GnRH, which stimulates their secretion and release into the bloodstream. The pulsating nature of the secretion of FSH and LH is a consequence of “direct signals” from the hypothalamus. The frequency and amplitude of GnRH secretion pulses changes depending on the phases of the menstrual cycle and affects the concentration and ratio of FSH/LH in the blood plasma.
FSH stimulates the growth of follicles and egg maturation in the ovary, the proliferation of granulosa cells, the formation of FSH and LH receptors on the surface of granulosa cells, the activity of aromatase in the ripening follicle (this enhances the conversion of androgens to estrogens), the production of inhibin, activin and insulin-like growth factors.
LH promotes the formation of androgens in theca cells, ensures ovulation (together with FSH), stimulates the synthesis of progesterone in luteinized granulosa cells (corpus luteum) after ovulation.
Prolactin has a variety of effects on a woman’s body. Its main biological role is stimulation of mammary gland growth, regulation of lactation; it also has a fat-mobilizing and hypotensive effect, controls the secretion of progesterone by the corpus luteum by activating the formation of LH receptors in it. During pregnancy and lactation, the level of prolactin in the blood increases. Hyperprolactinemia leads to impaired growth and maturation of follicles in the ovary (anovulation).
Posterior pituitary gland (neurohypophysis) is not an endocrine gland, but only deposits hypothalamic hormones (oxytocin and vasopressin), which are found in the body in the form of a protein complex.
Ovaries relate to the fourth level regulation of the reproductive system and perform two main functions. In the ovaries, cyclical growth and maturation of follicles and egg maturation occur, i.e. the generative function is carried out, as well as the synthesis of sex steroids (estrogens, androgens, progesterone) - a hormonal function.
The main morphofunctional unit of the ovary is follicle. At birth, a girl’s ovaries contain approximately 2 million primordial follicles. The majority of them (99%) undergo atresia (reverse development of follicles) during their lives. Only a very small part of them (300-400) goes through the full development cycle - from primordial to preovulatory with the subsequent formation of the corpus luteum. By the time of menarche, the ovaries contain 200-400 thousand primordial follicles.
The ovarian cycle consists of two phases: follicular and luteal. Follicular phase begins after menstruation, associated with growth
and maturation of follicles and ends with ovulation. Luteal phase occupies the period after ovulation until the onset of menstruation and is associated with the formation, development and regression of the corpus luteum, the cells of which secrete progesterone.
Depending on the degree of maturity, four types of follicle are distinguished: primordial, primary (preantral), secondary (antral) and mature (preovulatory, dominant) (Fig. 2.2).
Rice. 2.2. Structure of the ovary (diagram). Stages of development of the dominant follicle and corpus luteum: 1 - ovarian ligament; 2 - tunica albuginea; 3 - ovarian vessels (terminal branch of the ovarian artery and vein); 4 - primordial follicle; 5 - preantral follicle; 6 - antral follicle; 7 - preovulatory follicle; 8 - ovulation; 9 - yellow body; 10 - white body; 11 - egg (oocyte); 12 - basement membrane; 13 - follicular fluid; 14 - egg-bearing tubercle; 15 - theca-shell; 16 - shiny shell; 17 - granulosa cells
Primordial follicle consists of an immature egg (oocyte) in prophase of the 2nd meiotic division, which is surrounded by a single layer of granulosa cells.
IN preantral (primary) follicle The oocyte increases in size. Granulosa epithelial cells proliferate and round to form the granular layer of the follicle. A connective tissue membrane, the theca, is formed from the surrounding stroma (theca).
Antral (secondary) follicle characterized by further growth: the proliferation of cells of the granulosa layer, which produce follicular fluid, continues. The resulting fluid pushes the egg to the periphery, where the cells of the granular layer form the egg-bearing tubercle (cumulus oophorus). The connective tissue membrane of the follicle is clearly differentiated into outer and inner. Inner shell (the-ca interna) consists of 2-4 layers of cells. Outer shell (theca externa) located above the internal one and is represented by a differentiated connective tissue stroma.
IN preovulatory (dominant) follicle the egg, located on the ovarian tubercle, is covered with a membrane called the zona pellucida (zona pellucida). In the oocyte of the dominant follicle, the process of meiosis resumes. During maturation, a hundredfold increase in the volume of follicular fluid occurs in the preovulatory follicle (follicle diameter reaches 20 mm) (Fig. 2.3).
During each menstrual cycle, 3 to 30 primordial follicles begin to grow, becoming preantral (primary) follicles. In the subsequent menstrual cycle, folliculogenesis continues and only one follicle develops from preantral to preovulatory. During the growth of the follicle from preantral to antral

Rice. 2.3. Dominant follicle in the ovary. Laparoscopy
Granulosa cells synthesize anti-Mullerian hormone, which promotes its development. The remaining follicles that initially began to grow undergo atresia (degeneration).
Ovulation - rupture of the preovulatory (dominant) follicle and release of the egg into the abdominal cavity. Ovulation is accompanied by bleeding from the destroyed capillaries surrounding theca cells (Fig. 2.4).
After the release of the egg, the resulting capillaries quickly grow into the remaining cavity of the follicle. Granulosa cells undergo luteinization, which is morphologically manifested in an increase in their volume and the formation of lipid inclusions - the formation of corpus luteum(Fig. 2.5).

Rice. 2.4. Ovarian follicle after ovulation. Laparoscopy

Rice. 2.5. Corpus luteum of the ovary. Laparoscopy
Corpus luteum - a transient hormonally active formation that functions for 14 days, regardless of the total duration of the menstrual cycle. If pregnancy does not occur, the corpus luteum regresses, but if fertilization occurs, it functions until the formation of the placenta (12th week of pregnancy).
Hormonal function of the ovaries
The growth and maturation of follicles in the ovaries and the formation of the corpus luteum are accompanied by the production of sex hormones by both the granulosa cells of the follicle and the cells of the theca interna and, to a lesser extent, the theca externa. Sex steroid hormones include estrogens, progesterone and androgens. The starting material for the formation of all steroid hormones is cholesterol. Up to 90% of steroid hormones are in a bound state and only 10% of unbound hormones exert their biological effect.
Estrogens are divided into three fractions with different activities: estradiol, estriol, estrone. Estrone is the least active fraction, secreted by the ovaries mainly during the aging period - postmenopause; the most active fraction is estradiol, it is significant in the onset and maintenance of pregnancy.
The amount of sex hormones changes throughout the menstrual cycle. As the follicle grows, the synthesis of all sex hormones increases, but mainly estrogens. In the period after ovulation and before the onset of menstruation, progesterone is predominantly synthesized in the ovaries, secreted by the cells of the corpus luteum.
Androgens (androstenedione and testosterone) are produced by the follicle cells and interstitial cells. Their level does not change throughout the menstrual cycle. Once in granulosa cells, androgens actively undergo aromatization, leading to their conversion into estrogens.
In addition to steroid hormones, the ovaries also secrete other biologically active compounds: prostaglandins, oxytocin, vasopressin, relaxin, epidermal growth factor (EGF), insulin-like growth factors (IGF-1 and IGF-2). It is believed that growth factors contribute to the proliferation of granulosa cells, the growth and maturation of the follicle, and the selection of the dominant follicle.
In the process of ovulation, prostaglandins (F 2a and E 2), as well as proteolytic enzymes, collagenase, oxytocin, and relaxin contained in the follicular fluid, play a certain role.
Cyclical activity of the reproductive system is determined by the principles of direct and feedback, which is provided by specific receptors for hormones in each of the links. The direct connection is the stimulating effect of the hypothalamus on the pituitary gland and the subsequent formation of sex steroids in the ovary. Feedback is determined by the influence of increased concentrations of sex steroids on higher levels, blocking their activity.
In the interaction of parts of the reproductive system, “long”, “short” and “ultra-short” loops are distinguished. The “long” loop is the effect through the receptors of the hypothalamic-pituitary system on the production of sex hormones. The “short” loop defines the connection between the pituitary gland and the hypothalamus, the “ultra-short” loop determines the connection between the hypothalamus and nerve cells, which, under the influence of electrical stimuli, carry out local regulation with the help of neurotransmitters, neuropeptides, and neuromodulators.
Follicular phase
Pulsatile secretion and release of GnRH leads to the release of FSH and LH from the anterior pituitary gland. LH promotes the synthesis of androgens by the follicle cells. FSH acts on the ovaries and leads to follicle growth and oocyte maturation. At the same time, the increasing level of FSH stimulates the production of estrogens in granulosa cells by aromatizing androgens formed in the follicle cells, and also promotes the secretion of inhibin and IGF-1-2. Before ovulation, the number of receptors for FSH and LH in theca and granulosa cells increases (Fig. 2.6).
Ovulation occurs in the middle of the menstrual cycle, 12-24 hours after reaching the peak of estradiol, causing an increase in the frequency and amplitude of GnRH secretion and a sharp preovulatory rise in LH secretion according to the “positive feedback” type. Against this background, proteolytic enzymes - collagenase and plasmin - are activated, destroying the collagen of the follicle wall and thus reducing its strength. At the same time, the observed increase in the concentration of prostaglandin F 2a, as well as oxytocin, induces rupture of the follicle as a result of their stimulation of smooth muscle contraction and expulsion of the oocyte with the egg-bearing tubercle from the follicle cavity. The rupture of the follicle is also facilitated by an increase in the concentration of prostaglandin E 2 and relaxin in it, which reduce the rigidity of its walls.
Luteal phase
After ovulation, LH levels decrease relative to the “ovulatory peak.” However, this amount of LH stimulates the process of luteinization of granulosa cells remaining in the follicle, as well as the preferential secretion of progesterone by the resulting corpus luteum. Maximum secretion of progesterone occurs on the 6-8th day of the existence of the corpus luteum, which corresponds to the 20-22nd day of the menstrual cycle. Gradually, by the 28-30th day of the menstrual cycle, the level of progesterone, estrogen, LH and FSH decreases, the corpus luteum regresses and is replaced by connective tissue (corpus alba).
Fifth level The regulation of reproductive function consists of target organs that are sensitive to fluctuations in the level of sex steroids: the uterus, fallopian tubes, vaginal mucosa, as well as mammary glands, hair follicles, bones, adipose tissue, and the central nervous system.
Ovarian steroid hormones affect metabolic processes in organs and tissues that have specific receptors. These receptors may be

Rice. 2.6. Hormonal regulation of the menstrual cycle (scheme): a - changes in hormone levels; b - changes in the ovary; c - changes in the endometrium
both cytoplasmic and nuclear. Cytoplasmic receptors are strictly specific to estrogens, progesterone and testosterone. Steroids penetrate target cells by binding to specific receptors - estrogen, progesterone, testosterone, respectively. The resulting complex enters the cell nucleus, where, combining with chromatin, it ensures the synthesis of specific tissue proteins through the transcription of messenger RNA.
Uterus consists of the outer (serous) covering, myometrium and endometrium. The endometrium morphologically consists of two layers: basal and functional. The basal layer does not change significantly during the menstrual cycle. The functional layer of the endometrium undergoes structural and morphological changes, manifested by a successive change of stages proliferation, secretion, desquamation followed by
regeneration. Cyclic secretion of sex hormones (estrogens, progesterone) leads to biphasic changes in the endometrium, aimed at the perception of a fertilized egg.
Cyclic changes in the endometrium touch its functional (surface) layer, consisting of compact epithelial cells, which are rejected during menstruation. The basal layer, which is not rejected during this period, ensures the restoration of the functional layer.
The following changes occur in the endometrium during the menstrual cycle: desquamation and rejection of the functional layer, regeneration, proliferation phase and secretion phase.
Transformation of the endometrium occurs under the influence of steroid hormones: the proliferation phase - under the predominant action of estrogens, the secretion phase - under the influence of progesterone and estrogens.
Proliferation phase(corresponds to the follicular phase in the ovaries) lasts an average of 12-14 days, starting from the 5th day of the cycle. During this period, a new surface layer is formed with elongated tubular glands lined with columnar epithelium with increased mitotic activity. The thickness of the functional layer of the endometrium is 8 mm (Fig. 2.7).
Secretion phase (luteal phase in the ovaries) associated with the activity of the corpus luteum, lasts 14±1 day. During this period, the epithelium of the endometrial glands begins to produce secretions containing acidic glycosaminoglycans, glycoproteins, and glycogen (Fig. 2.8).

Rice. 2.7. The endometrium is in the proliferation phase (middle stage). Hematoxylin and eosin staining, × 200. Photo by O.V. Zairatiantsa

Rice. 2.8. The endometrium is in the secretion phase (middle stage). Hematoxylin and eosin staining, ×200. Photo by O.V. Zairatiantsa
Secretion activity becomes highest on the 20-21st day of the menstrual cycle. By this time, the maximum amount of proteolytic enzymes is found in the endometrium, and decidual transformations occur in the stroma. A sharp vascularization of the stroma is noted - the spiral arteries of the functional layer are tortuous, forming “tangles”, the veins are dilated. Such changes in the endometrium, noted on days 20-22 (days 6-8 after ovulation) of the 28-day menstrual cycle, provide the best conditions for implantation of a fertilized egg.
By the 24-27th day, due to the onset of regression of the corpus luteum and a decrease in the concentration of progesterone produced by it, the endometrial trophism is disrupted, and gradually increases in it degenerative changes. Granules containing relaxin are secreted from the granular cells of the endometrial stroma, which prepares menstrual rejection of the mucous membrane. In the superficial areas of the compact layer, lacunar expansion of capillaries and hemorrhages into the stroma are noted, which can be detected 1 day before the onset of menstruation.
Menstruation includes desquamation, rejection and regeneration of the functional layer of the endometrium. Due to regression of the corpus luteum and a sharp decrease in the content of sex steroids in the endometrium, hypoxia increases. The onset of menstruation is facilitated by prolonged spasm of the arteries, leading to blood stasis and the formation of blood clots. Tissue hypoxia (tissue acidosis) is aggravated by increased endothelial permeability, fragility of vessel walls, numerous small hemorrhages and massive leukemia.
cytic infiltration. Lysosomal proteolytic enzymes released from leukocytes enhance the melting of tissue elements. Following a prolonged spasm of blood vessels, their paretic dilation occurs with increased blood flow. At the same time, there is an increase in hydrostatic pressure in the microcirculatory bed and rupture of the walls of blood vessels, which by this time have largely lost their mechanical strength. Against this background, active desquamation of necrotic areas of the functional layer of the endometrium occurs. By the end of the 1st day of menstruation, 2/3 of the functional layer is rejected, and its complete desquamation usually ends on the 3rd day of the menstrual cycle.
Regeneration of the endometrium begins immediately after the rejection of the necrotic functional layer. The basis for regeneration are the epithelial cells of the stroma of the basal layer. Under physiological conditions, already on the 4th day of the cycle, the entire wound surface of the mucous membrane is epithelialized. This is again followed by cyclic changes in the endometrium - the phases of proliferation and secretion.
Consecutive changes throughout the cycle in the endometrium - proliferation, secretion and menstruation - depend not only on cyclic fluctuations in the level of sex steroids in the blood, but also on the state of tissue receptors for these hormones.
The concentration of nuclear estradiol receptors increases until the middle of the cycle, reaching a peak towards the late period of the endometrial proliferation phase. After ovulation, there is a rapid decrease in the concentration of nuclear estradiol receptors, continuing until the late secretory phase, when their expression becomes significantly lower than at the beginning of the cycle.
Functional status fallopian tubes varies depending on the phase of the menstrual cycle. Thus, in the luteal phase of the cycle, the ciliated apparatus of the ciliated epithelium and the contractile activity of the muscular layer are activated, aimed at optimal transport of sex gametes into the uterine cavity.
Changes in extragenital target organs
All sex hormones not only determine functional changes in the reproductive system itself, but also actively influence metabolic processes in other organs and tissues that have receptors for sex steroids.
In the skin, under the influence of estradiol and testosterone, collagen synthesis is activated, which helps maintain its elasticity. Increased oiliness, acne, folliculitis, skin porosity and excess hair growth occur when androgen levels increase.
In bone, estrogens, progesterone and androgens support normal remodeling by preventing bone resorption. The balance of sex steroids affects the metabolism and distribution of adipose tissue in the female body.
The effect of sex hormones on receptors in the central nervous system and hippocampal structures is associated with changes in the emotional sphere and vegetative
reactions in a woman in the days preceding menstruation - the phenomenon of the “menstrual wave”. This phenomenon is manifested by an imbalance in the processes of activation and inhibition in the cerebral cortex, fluctuations in the sympathetic and parasympathetic nervous system(especially affecting the cardiovascular system). External manifestations These fluctuations are caused by mood changes and irritability. In healthy women, these changes do not go beyond physiological boundaries.
The influence of the thyroid gland and adrenal glands on reproductive function
Thyroid produces two iodamine acid hormones - triiodothyronine (T 3) and thyroxine (T 4), which are the most important regulators of metabolism, development and differentiation of all body tissues, especially thyroxine. Thyroid hormones have a certain effect on the protein-synthetic function of the liver, stimulating the formation of globulin that binds sex steroids. This is reflected in the balance of free (active) and bound ovarian steroids (estrogens, androgens).
With a lack of T 3 and T 4, the secretion of thyrotropin-releasing hormone increases, activating not only thyrotrophs, but also lactotrophs of the pituitary gland, which often becomes the cause of hyperprolactinemia. In parallel, the secretion of LH and FSH decreases with inhibition of folliculo- and steroidogenesis in the ovaries.
An increase in the level of T 3 and T 4 is accompanied by a significant increase in the concentration of globulin, which binds sex hormones in the liver and leads to a decrease in the free estrogen fraction. Hypoestrogenism, in turn, leads to impaired follicle maturation.
Adrenal glands. Normally, the production of androgens - androstenedione and testosterone - in the adrenal glands is the same as in the ovaries. DHEA and DHEA-S are produced in the adrenal glands, while these androgens are practically not synthesized in the ovaries. DHEA-S, secreted in the largest amount (compared to other adrenal androgens), has relatively low androgenic activity and serves as a kind of reserve form of androgens. Adrenal androgens, along with androgens of ovarian origin, are the substrate for extragonadal estrogen production.
Assessment of the state of the reproductive system according to functional diagnostic tests
For many years, so-called functional diagnostic tests for the state of the reproductive system have been used in gynecological practice. The value of these fairly simple studies has remained to this day. The most commonly used are measurement of basal temperature, assessment of the “pupil” phenomenon and the state of cervical mucus (its crystallization, distensibility), as well as calculation of the karyopyknotic index (KPI, %) of the vaginal epithelium (Fig. 2.9).

Rice. 2.9. Functional diagnostic tests for a two-phase menstrual cycle
Basal temperature test is based on the ability of progesterone (in increased concentration) to directly affect the thermoregulation center in the hypothalamus. Under the influence of progesterone, a transient hyperthermic reaction occurs in the 2nd (luteal) phase of the menstrual cycle.
The patient measures the temperature in the rectum daily in the morning without getting out of bed. The results are displayed graphically. With a normal two-phase menstrual cycle, the basal temperature in the 1st (follicular) phase of the menstrual cycle does not exceed 37 °C, in the 2nd (luteal) phase there is an increase in rectal temperature by 0.4-0.8 °C compared to the initial value . On the day of menstruation or 1 day before its onset, the corpus luteum in the ovary regresses, the level of progesterone decreases, and therefore the basal temperature drops to its original values.
A persistent two-phase cycle (basal temperature must be measured over 2-3 menstrual cycles) indicates that ovulation has occurred and the functional usefulness of the corpus luteum. The absence of a rise in temperature in the 2nd phase of the cycle indicates the absence of ovulation (anovulation); delay in the rise, its short duration (increase in temperature for 2-7 days) or insufficient rise (by 0.2-0.3 °C) - on the defective function of the corpus luteum, i.e. insufficiency of progesterone production. A false positive result (an increase in basal temperature in the absence of the corpus luteum) is possible with acute and chronic infections, with some changes in the central nervous system, accompanied by increased excitability.
"Pupil" symptom reflects the amount and condition of mucous secretion in the cervical canal, which depend on the estrogen saturation of the body. The “pupil” phenomenon is based on the expansion of the external os of the cervical canal due to the accumulation of transparent glassy mucus in it and is assessed when examining the cervix using vaginal speculum. Depending on the severity of the “pupil” symptom, it is assessed in three degrees: +, ++, +++.
The synthesis of cervical mucus during the 1st phase of the menstrual cycle increases and becomes maximum immediately before ovulation, which is associated with a progressive increase in estrogen levels during this period. On preovulatory days, the dilated external opening of the cervical canal resembles a pupil (+++). In the 2nd phase of the menstrual cycle, the amount of estrogen decreases, progesterone is predominantly produced in the ovaries, so the amount of mucus decreases (+), and before menstruation it is completely absent (-). The test cannot be used for pathological changes in the cervix.
Symptom of crystallization of cervical mucus(the "fern" phenomenon) When dried, it is most pronounced during ovulation, then crystallization gradually decreases, and before menstruation it is completely absent. Crystallization of mucus dried in air is also assessed in points (from 1 to 3).
Symptom of cervical mucus tension is directly proportional to the level of estrogen in the female body. To carry out the test, mucus is removed from the cervical canal using a forceps, the jaws of the instrument are slowly moved apart, determining the degree of tension (the distance at which the mucus “breaks”). The maximum stretching of cervical mucus (up to 10-12 cm) occurs during the period of the highest concentration of estrogen - in the middle of the menstrual cycle, which corresponds to ovulation.
Mucus can be negatively affected by inflammatory processes in the genital organs, as well as hormonal imbalances.
Karyopyknotic index(KPI). Under the influence of estrogens, the cells of the basal layer of the stratified squamous epithelium of the vagina proliferate, and therefore the number of keratinizing (peeling, dying) cells in the surface layer increases. The first stage of cell death is changes in their nucleus (karyopyknosis). KPI is the ratio of the number of cells with a pyknotic nucleus (i.e., keratinizing) to the total number of epithelial cells in the smear, expressed as a percentage. At the beginning of the follicular phase of the menstrual cycle, the CPI is 20-40%; on preovulatory days it increases to 80-88%, which is associated with a progressive increase in estrogen levels. In the luteal phase of the cycle, the level of estrogen decreases, therefore, the CPI decreases to 20-25%. Thus, the quantitative ratios of cellular elements in smears of the vaginal mucosa make it possible to judge the saturation of the body with estrogen.
Currently, especially in the in vitro fertilization (IVF) program, follicle maturation, ovulation and the formation of the corpus luteum are determined by dynamic ultrasound.
Control questions
1. Describe the normal menstrual cycle.
2. Indicate the levels of regulation of the menstrual cycle.
3. List the principles of feedforward and feedback.
4. What changes occur in the ovaries during the normal menstrual cycle?
5. What changes occur in the uterus during a normal menstrual cycle?
6. Name the functional diagnostic tests.
Gynecology: textbook / B. I. Baisova et al.; edited by G. M. Savelyeva, V. G. Breusenko. - 4th ed., revised. and additional - 2011. - 432 p. : ill.
List of abbreviations:
ADH - antidiuretic hormone
ACTH - corticoliberin
ARG-Gn - agonist of gonadotropin releasing hormone
LH - luteinizing hormone
OP - oxyprogesterone
RG-Gn - gonadotropin releasing hormone
STH - somatoliberin
VEGF - vascular endothelial growth factor
TSH - thyroid stimulating hormone (thyrotropin-releasing hormone)
FSH - follicle stimulating hormone
FGF - fibroplastic growth factor
Normal menstrual cycle
Menses is a bloody discharge from a woman’s genital tract that periodically occurs as a result of rejection of the functional layer of the endometrium at the end of a two-phase menstrual cycle.
The complex of cyclic processes that occur in the female body and are externally manifested by menstruation is called the menstrual cycle. Menstruation begins as a response to changes in the level of steroids produced by the ovaries.
Clinical signs of a normal menstrual cycleThe duration of the menstrual cycle during a woman’s active reproductive period is on average 28 days. A cycle length of 21 to 35 days is considered normal. Large intervals are observed during puberty and menopause, which may be a manifestation of anovulation, which can be observed most often at this time.
Typically, menstruation lasts from 3 to 7 days, the amount of blood lost is insignificant. Shortening or prolongation of menstrual bleeding, as well as the appearance of scanty or heavy menstruation, can serve as a manifestation of a number of gynecological diseases.
Characteristics of a normal menstrual cycle:
Duration: 28±7 days;
Duration of menstrual bleeding: 4±2 days;
Volume of blood loss during menstruation: 20-60 ml * ;
Average iron loss: 16 mg
*
95 percent of healthy women lose less than 60 ml of blood with each menstruation. Blood loss of more than 60-80 ml is combined with a decrease in the level of hemoglobin, hematocrit and serum iron.
Physiology of menstrual bleeding:
Immediately before menstruation, a pronounced spasm of the spiral arterioles develops. After dilatation of the spiral arterioles, menstrual bleeding begins. At first, platelet adhesion in endometrial vessels is suppressed, but then, as blood transudates, the damaged ends of the vessels are sealed with intravascular thrombi consisting of platelets and fibrin. 20 hours after the onset of menstruation, when most of the endometrium has already been rejected, a pronounced spasm of the spiral arterioles develops, due to which hemostasis is achieved. Regeneration of the endometrium begins 36 hours after the onset of menstruation, despite the fact that the rejection of the endometrium is not yet completely completed.
Regulation of the menstrual cycle is a complex neurohumoral mechanism, which is carried out with the participation of 5 main links of regulation. These include: the cerebral cortex, subcortical centers (hypothalamus), pituitary gland, gonads, peripheral organs and tissues (uterus, fallopian tubes, vagina, mammary glands, hair follicles, bones, adipose tissue). The latter are called target organs, due to the presence of receptors sensitive to the action of hormones that the ovary produces during the menstrual cycle. Cytosol receptors are cytoplasmic receptors that have strict specificity for estradiol, progesterone, and testosterone, while nuclear receptors can be acceptors of molecules such as insulin, glucagon, and aminopeptides.
Receptors for sex hormones are found in all structures of the reproductive system, as well as in the central nervous system, skin, adipose and bone tissue and mammary gland. A free steroid hormone molecule is captured by a specific cytosol receptor of a protein nature, and the resulting complex is translocated into the cell nucleus. A new complex with a nuclear protein receptor appears in the nucleus; this complex binds to chromatin, which regulates the transcription of mRNA and is involved in the synthesis of specific tissue proteins. The intracellular mediator, cyclic adenosine monophosphoric acid (cAMP), regulates metabolism in target tissue cells in accordance with the needs of the body in response to hormones. The bulk of steroid hormones (about 80% is in the blood and transported in bound form. Their transport is carried out by special proteins - steroid-binding globulins and nonspecific transport systems (albumin and erythrocytes). In bound form, steroids are inactive, therefore globulins, albumins and erythrocytes can be considered as a kind of buffer system that controls the access of steroids to the receptors of target cells.
Cyclic functional changes occurring in a woman’s body can be divided into changes in the hypothalamic-pituitary-ovarian system (ovarian cycle) and the uterus, primarily in its mucous membrane (uterine cycle).
Along with this, as a rule, cyclical changes occur in all organs and systems of a woman, in particular in the central nervous system, cardiovascular system, thermoregulation system, metabolic processes, etc.
Hypothalamus
The hypothalamus is the part of the brain located above the optic chiasm and forming the bottom of the third ventricle. It is an old and stable component of the central nervous system, the general organization of which has changed little during human evolution. Structurally and functionally, the hypothalamus is connected to the pituitary gland. There are three hypothalamic regions: anterior, posterior and intermediate. Each region is formed by nuclei - clusters of neuron bodies of a certain type.
In addition to the pituitary gland, the hypothalamus influences the limbic system (amygdala, hippocampus), thalamus, and pons. These departments also directly or indirectly influence the hypothalamus.
The hypothalamus secretes liberins and statins. This process is regulated by hormones that close three feedback loops: long, short and ultrashort. A long feedback loop is provided by circulating sex hormones that bind to the corresponding receptors in the hypothalamus, a short feedback loop is provided by adenohypophysis hormones, and an ultra-short feedback loop is provided by liberins and statins. Liberins and statins regulate the activity of the adenohypophysis. Gonadotropin-releasing hormone stimulates the secretion of LH and FSH, corticoliberin - ACTH, somatoliberin (STH), thyrotropin-releasing hormone (TSH). In addition to liberins and statins, antidiuretic hormone and oxytocin are synthesized in the hypothalamus. These hormones are transported to the neurohypophysis, from where they enter the blood.
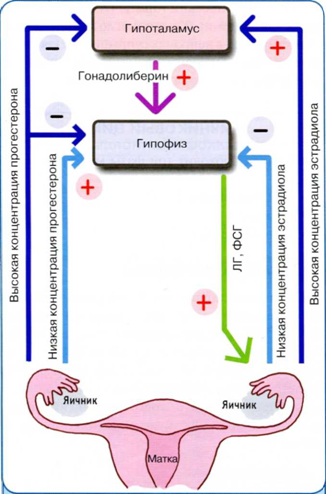
Unlike the capillaries of other areas of the brain, the capillaries of the hypothalamic infundibulum are fenestrated. They form the primary capillary network of the gate system.
In the 70-80s. A series of experimental studies were carried out on monkeys, which made it possible to identify differences in the function of the neurosecretory structures of the hypothalamus of primates and rodents. In primates and humans, the arcuate nuclei of the mediobasal hypothalamus are the only place of formation and release of RH-LH, which is responsible for the gonadotropic function of the pituitary gland. The secretion of RH-LH is genetically programmed and occurs in a certain pulsating rhythm with a frequency of approximately once per hour. This rhythm is called circhoral (clockwise). The area of the arcuate nuclei of the hypothalamus is called the arcuate oscillator. The circhoral nature of LH-RH secretion was confirmed by direct determination of it in the blood of the portal system of the pituitary stalk and jugular vein in monkeys and in the blood of women with an ovulatory cycle.
Hypothalamic hormones
LH releasing hormone has been isolated, synthesized and described in detail. To date, it has not been possible to isolate and synthesize folliberin. LH-RH and its synthetic analogues have the ability to stimulate the release of LH and FSH from the anterior pituitary gland, so one term has now been adopted for hypothalamic gonadotropic liberins - gonadotropin-releasing hormone (RH-Gn).
GnRH stimulates the secretion of FSH and LH. It is a decapeptide secreted by neurons of the infundibulum nucleus. GnRH is not secreted constantly, but in a pulsed manner. It is very quickly destroyed by proteases (half-life is 2-4 minutes), so its impulses must be regular. The frequency and amplitude of GnRH releases change throughout the menstrual cycle. The follicular phase is characterized by frequent fluctuations of small amplitude in the level of GnRH in the blood serum. Towards the end of the follicular phase, the frequency and amplitude of oscillations increase and then decrease during the luteal phase.
Pituitary
The pituitary gland has two lobes: the anterior - adenohypophysis and the posterior - neurohypophysis. The neurohypophysis is of neurogenic origin and represents a continuation of the hypothalamic infundibulum. The neurohypophysis is supplied with blood from the inferior pituitary arteries. The adenohypophysis develops from the ectoderm of Rathke's pouch, therefore it consists of glandular epithelium and does not have a direct connection with the hypothalamus. Liberins and statins synthesized in the hypothalamus enter the adenohypophysis through a special portal system. This is the main source of blood supply to the adenohypophysis. Blood enters the portal system primarily through the superior pituitary arteries. In the area of the hypothalamic infundibulum, they form the primary capillary network of the portal system, from which the portal veins are formed, which enter the adenohypophysis and give rise to the secondary capillary network. Reverse blood flow through the portal system is possible. The peculiarities of the blood supply and the absence of the blood-brain barrier in the area of the hypothalamic infundibulum provide a two-way connection between the hypothalamus and the pituitary gland. Depending on the staining with hematoxylin and eosin, the secretory cells of the adenohypophysis are divided into chromophilic (acidophilic) and basophilic (chromophobic). Acidophilic cells secrete GH and prolactin, basophilic cells secrete FSH, LH, TSH, ACTH.
Pituitary hormones
The adenohypophysis produces growth hormone, prolactin, FSH, LH, TSH and ACTH. FSH and LH regulate the secretion of sex hormones, TSH - the secretion of thyroid hormones, ACTH - the secretion of hormones from the adrenal cortex. HGH stimulates growth and has an anabolic effect. Prolactin stimulates the growth of mammary glands during pregnancy and lactation after childbirth.
LH and FSH are synthesized by gonadotropic cells of the adenohypophysis and play an important role in the development of ovarian follicles. By structure they belong to glycoproteins. FSH stimulates follicle growth, proliferation of granulosa cells, and induces the formation of LH receptors on the surface of granulosa cells. Under the influence of FSH, the content of aromatase in the ripening follicle increases. LH stimulates the formation of androgens (precursors of estrogens) in theca cells, together with FSH promotes ovulation and stimulates the synthesis of progesterone in the luteinized granulosa cells of the ovulated follicle.
The secretion of LH and FSH is variable and modulated by ovarian hormones, especially estrogens and progesterone.
Thus, low level estrogen has a suppressive effect on LH, while high estrogen stimulates its production by the pituitary gland. In the late follicular phase, the level of serum estrogens is quite high, the positive feedback effect is tripled, which contributes to the formation of a preovulatory LH peak. And, conversely, during therapy with combined contraceptives, the level of estrogen in the blood serum is within the limits that determine negative feedback, which leads to a decrease in the content of gonadotropins.
The positive feedback mechanism leads to an increase in the concentration and production of RG-Gn in the receptors.
In contrast to the effect of estrogens, low progesterone levels have a positive feedback reaction on the secretion of LH and FSH by the pituitary gland. Such conditions exist just before ovulation and lead to the release of FSH. The high level of progesterone, which is observed in the luteal phase, reduces the pituitary production of gonadotropins. A small amount of progesterone stimulates the release of gonadotropins at the level of the pituitary gland. The negative feedback effect of progesterone occurs by reducing the production of GnRH and reducing the sensitivity to GnRH at the level of the pituitary gland. Positive feedback effects of progesterone occur on the pituitary gland and include increased sensitivity to RH-Gn. Estrogens and progesterone are not the only hormones that affect the secretion of gonadotropins by the pituitary gland. The hormones inhibin and activin have the same effect. Inhibin suppresses pituitary FSH secretion, activin stimulates it.
Prolactin is a polypeptide consisting of 198 amino acid residues, synthesized by lactotropic cells of the adenohypophysis. The secretion of prolactin is controlled by dopamine. It is synthesized in the hypothalamus and inhibits the secretion of prolactin. Prolactin has a variety of effects on a woman’s body. Its main biological role is the growth of mammary glands and the regulation of lactation. It also has a fat-mobilizing effect and has a hypotensive effect. An increase in prolactin secretion is one of the common causes of infertility, since an increase in its level in the blood inhibits steroidogenesis in the ovaries and the development of follicles.
Oxytocin- a peptide consisting of 9 amino acid residues. It is formed in the neurons of the magnocellular part of the paraventricular nuclei of the hypothalamus. The main targets of oxytocin in humans are the smooth muscle fibers of the uterus and myoepithelial cells of the mammary glands.
Antidiuretic hormone(ADG) is a peptide consisting of 9 amino acid residues. Synthesized in neurons of the supraoptic nucleus of the hypothalamus. The main function of ADH is the regulation of blood volume, blood pressure, and plasma osmolality.
Ovarian cycle
The ovaries undergo three phases of the menstrual cycle:
- follicular phase;
- ovulation;
- luteal phase.
Follicular phase:
One of the main points of the follicular phase of the menstrual cycle is the development of the egg. A woman’s ovary is a complex organ consisting of many components, as a result of the interaction of which sex steroid hormones are secreted and an egg ready for fertilization is formed in response to the cyclic secretion of gonadotropins.
Steroidogenesis
Hormonal activity from the preantral to periovulatory follicle has been described as the "two cells, two gonadotropins" theory. Steroidogenesis occurs in two follicle cells: the theca and granulosa cells. In the theca cells, LH stimulates the production of androgens from cholesterol. In granulosa cells, FSH stimulates the conversion of resulting androgens into estrogens (aromatization). In addition to its aromatization effect, FSH is also responsible for the proliferation of granulosa cells. Although other mediators in the development of ovarian follicles are known, this theory is fundamental for understanding the processes occurring in the ovarian follicle. It has been revealed that both hormones are necessary for a normal cycle with sufficient levels of estrogen.
The production of androgens in the follicles can also regulate the development of the preantral follicle. A low level of androgens enhances the aromatization process, therefore, increases the production of estrogen, and vice versa, a high level inhibits the aromatization process and causes follicular atresia. A balance of FSH and LH is essential for early follicular development. The optimal condition for the initial stage of follicle development is a low level of LH and high FSH, which occurs at the beginning of the menstrual cycle. If LH levels are high, the theca cells produce large amounts of androgens, causing follicular atresia.
Choosing a dominant follicle
The growth of the follicle is accompanied by the secretion of sex steroid hormones under the influence of LH and FSH. These gonadotropins protect the group of preantral follicles from atresia. However, normally only one of these follicles develops into a preovulatory follicle, which is then released and becomes dominant.
The dominant follicle in the middle follicular phase is the largest and most developed in the ovary. Already in the first days of the menstrual cycle, it has a diameter of 2 mm and within 14 days by the time of ovulation it increases to an average of 21 mm. During this time, there is a 100-fold increase in the volume of follicular fluid, the number of granulosa cells lining the basement membrane increases from 0.5x10 6 to 50x10 6. This follicle has the highest aromatizing activity and the highest concentration of FSH-induced LH receptors, so the dominant follicle secretes the highest amount of estradiol and inhibin. Further, inhibin enhances the synthesis of androgens under the influence of LH, which is a substrate for the synthesis of estradiol.
Unlike the FSH level, which decreases as the concentration of estradiol increases, the LH level continues to increase (at low concentrations, estradiol inhibits the secretion of LH). It is long-term estrogen stimulation that prepares the ovulatory LH peak. At the same time, the dominant follicle is preparing for ovulation: under the local action of estrogens and FSH, the number of LH receptors on granulosa cells increases. The release of LH leads to ovulation, the formation of the corpus luteum and increased secretion of progesterone. Ovulation occurs 10-12 hours after the LH peak or 32-35 hours after its level begins to rise. Usually only one follicle ovulates.
During follicle selection, FSH levels decrease in response to the negative effects of estrogen, so the dominant follicle is the only one that continues to develop as FSH levels drop
The ovarian-pituitary connection is decisive in the selection of the dominant follicle and in the development of atresia of the remaining follicles.
Inhibin and activin
The growth and development of the egg and the functioning of the corpus luteum occur through the interaction of autocrine and paracrine mechanisms. It is necessary to note two follicular hormones that play a significant role in steroidogenesis - inhibin and activin.
Inhibin is a peptide hormone produced by granulosa cells of growing follicles that reduces the production of FSH. In addition, it affects the synthesis of androgens in the ovary. Inhibin affects folliculogenesis in the following way: reducing FSH to a level at which only the dominant follicle develops.
Activin is a peptide hormone produced in granulosa cells of the follicles and pituitary gland. According to some authors, activin is also produced by the placenta. Activin increases the production of FSH by the pituitary gland and enhances the process of FSH binding to granulosa cells.
Insulin-like growth factors
Insulin-like growth factors (IGF-1 and IGF-2) are synthesized in the liver under the influence of growth hormone and, possibly, in granulosa cells of follicles, and act as paracrine regulators. Before ovulation, the content of IGF-1 and IGF-2 in the follicular fluid increases due to an increase in the amount of fluid itself in the dominant follicle. IGF-1 is involved in the synthesis of estradiol. IGF-2 (epidermal) inhibits the synthesis of steroids in the ovaries.
Ovulation:
The ovulatory LH peak leads to an increase in the concentration of prostaglandins and protease activity in the follicle. The process of ovulation itself is a rupture of the basal membrane of the dominant follicle and bleeding from the destroyed capillaries surrounding the theca cells. Changes in the wall of the preovulatory follicle, causing its thinning and rupture, occur under the influence of the enzyme collagenase; Prostaglandins contained in follicular fluid, proteolytic enzymes formed in granulosa cells, oxytopin and relaxin also play a certain role. As a result, a small hole is formed in the wall of the follicle through which the egg is slowly released. Direct measurements showed that the pressure inside the follicle does not increase during ovulation.
At the end of the follicular phase, FSH acts on LH receptors in granulosa cells. Estrogens are an obligatory cofactor in this effect. As the dominant follicle develops, estrogen production increases. As a result, the production of estrogen is sufficient to achieve the secretion of LH by the pituitary gland, which leads to an increase in its level. The increase occurs very slowly at first (from the 8th to the 12th day of the cycle), then quickly (after the 12th day of the cycle). During this time, LH activates luteinization of granulosa cells in the dominant follicle. Thus, progesterone is released. Progesterone further enhances the effect of estrogen on the secretion of LH by the pituitary gland, leading to an increase in its level.
Ovulation occurs within 36 hours after the onset of the LH rise. Determination of LH surge is one of best methods, which determines ovulation and is carried out using an “ovulation detector” device.
The periovulatory FSH peak likely results from the beneficial effects of progesterone. In addition to increases in LH, FSH, and estrogens, serum androgens also increase during ovulation. These androgens are released as a result of the stimulating effect of LH on theca cells, especially in the non-dominant follicle.
An increase in androgen levels has the effect of increasing libido, confirming that this is the most fertile period for women.
LH levels stimulate meiosis after the sperm enters the egg. When an oocyte is released from the ovary during ovulation, the follicle wall is destroyed. This is regulated by LH, FSH and progesterone, which stimulate the activity of proteolytic enzymes such as plasminogen activators (which release plasmin, which stimulates collagenase activity) and prostaglandins. Prostaglandins not only increase the activity of proteolytic enzymes, but also contribute to the appearance of an inflammatory-like reaction in the follicle wall and stimulate the activity of smooth muscles, which promotes the release of the oocyte.
The importance of prostaglandins in the process of ovulation has been proven by studies that determine that a decrease in prostaglandin release can lead to a delay in the release of the oocyte from the ovary during normal steroidogenesis (non-developing luteinized follicle syndrome - SNLF). Since SNLF is often a cause of infertility, women wishing to become pregnant are advised to avoid taking synthesized prostaglandin inhibitors.
Luteal phase:
Structure of the corpus luteum
After the release of the egg from the ovary, the developing capillaries quickly grow into the follicle cavity; granulosa cells undergo luteinization: an increase in their cytoplasm and the formation of lipid inclusions. Granulosa cells and thekocytes form the corpus luteum - the main regulator of the luteal phase of the menstrual cycle. The cells that form the follicle wall accumulate lipids and the yellow pigment lutein and begin to secrete progesterone, estradiol-2, and inhibin. A powerful vascular network facilitates the entry of corpus luteum hormones into the systemic circulation. A full-fledged corpus luteum develops only in cases where an adequate number of granulosa cells with a high content of LH receptors are formed in the preovulatory follicle. The increase in the size of the corpus luteum after ovulation occurs mainly due to an increase in the size of granulosa cells, while their number does not increase due to the lack of mitoses. In humans, the corpus luteum secretes not only progesterone, but also estradiol and androgens. The mechanisms of regression of the corpus luteum have not been sufficiently studied. It is known that prostaglandins have a luteolytic effect.

Rice. Ultrasound picture of a “blooming” corpus luteum during 6 weeks of pregnancy. 4 days. Energy mapping mode.
Hormonal regulation of the luteal phase
If pregnancy does not occur, involution of the corpus luteum occurs. This process is regulated by a negative feedback mechanism: hormones (progesterone and estradiol) secreted by the corpus luteum act on the gonadotropic cells of the pituitary gland, suppressing the secretion of FSH and LH. Inhibin also suppresses FSH secretion. A decrease in FSH levels, as well as the local action of progesterone, prevents the development of a group of primordial follicles.
The existence of the corpus luteum depends on the level of LH secretion. When it decreases, usually 12-16 days after ovulation, involution of the corpus luteum occurs. A white body forms in its place. The mechanism of involution is unknown. Most likely, it is due to paracrine influences. As the corpus luteum involutes, the level of estrogen and progesterone falls, which leads to an increase in the secretion of gonadotropic hormones. As FSH and LH levels increase, a new group of follicles begins to develop.
If fertilization has occurred, the existence of the corpus luteum and the secretion of progesterone are supported by human chorionic gonadotropin. Thus, embryo implantation leads to hormonal changes that preserve the corpus luteum.
The duration of the luteal phase for most women is constant and is approximately 14 days.
Ovarian hormones
The complex process of steroid biosynthesis ends with the formation of estradiol, testosterone and progesterone. The steroid-producing tissues of the ovaries are granulosa cells lining the follicle cavity, theca interna cells and, to a much lesser extent, the stroma. Granulosa cells and theca cells synergistically participate in the synthesis of estrogens; theca cells are the main source of androgens, which are also produced in small quantities in the stroma; Progesterone is synthesized in theca cells and granulosa cells.
In the ovary, 60-100 mcg of estradiol (E2) is secreted in the early follicular phase of the menstrual cycle, 270 mcg in the luteal phase, and 400-900 mcg per day by the time of ovulation. About 10% of E2 is aromatized in the ovary from testosterone. The amount of estrone formed in the early follicular phase is 60-100 mcg; by the time of ovulation, its synthesis increases to 600 mcg per day. Only half the amount of estrone is produced in the ovary. The second half is flavored in E2. Estriol is a low-active metabolite of estradiol and estrone.
Progesterone is produced in the ovary in an amount of 2 mg/day in the follicular phase and 25 mg/day in the luteal phase of the menstrual cycle. During metabolism, progesterone in the ovary is converted into 20-dehydroprogesterone, which has relatively little biological activity.
The following androgens are synthesized in the ovary: androstenedione (a precursor of testosterone) in the amount of 1.5 mg/day (the same amount of androstenedione is produced in the adrenal glands). About 0.15 mg of testosterone is formed from androstenedione, approximately the same amount is formed in the adrenal glands.
Brief overview of the processes occurring in the ovaries
Follicular phase:
LH stimulates androgen production in theca cells.
FSH stimulates estrogen production in granulosa cells.
The most developed follicle in the middle of the follicular phase becomes dominant.
The increasing formation of estrogens and inhibin in the dominant follicle suppresses the release of FSH by the pituitary gland.
A decrease in FSH levels causes atresia of all follicles except the dominant one.
Ovulation:
FSH induces LH receptors.
Proteolytic enzymes in the follicle lead to the destruction of its wall and the release of the oocyte.
Luteal phase:
The corpus luteum is formed from granulosa and theca cells preserved after ovulation.
Progesterone, secreted by the corpus luteum, is the dominant hormone. In the absence of pregnancy, luteolysis occurs 14 days after ovulation.
Uterine cycle
The endometrium consists of two layers: functional and basal. The functional layer changes its structure under the influence of sex hormones and, if pregnancy does not occur, is rejected during menstruation.
Proliferative phase:
The beginning of the menstrual cycle is considered to be the 1st day of menstruation. At the end of menstruation, the thickness of the endometrium is 1-2 mm. The endometrium consists almost exclusively of the basal layer. The glands are narrow, straight and short, lined with low columnar epithelium; the cytoplasm of the stromal cells is almost indistinguishable. As estradiol levels increase, a functional layer is formed: the endometrium prepares for embryo implantation. The glands lengthen and become convoluted. The number of mitoses increases. As they proliferate, the height of the epithelial cells increases, and the epithelium itself changes from single-row to multirow by the time of ovulation. The stroma is swollen and loosened, with increased cell nuclei and cytoplasmic volume. The vessels are moderately tortuous.
Secretory phase:
Normally, ovulation occurs on the 14th day of the menstrual cycle. The secretory phase is characterized by high levels of estrogen and progesterone. However, after ovulation, the number of estrogen receptors in endometrial cells decreases. Endometrial proliferation is gradually inhibited, DNA synthesis decreases, and the number of mitoses decreases. Thus, progesterone has a predominant effect on the endometrium in the secretory phase.
Glycogen-containing vacuoles appear in the endometrial glands, which are detected using the PAS reaction. On the 16th day of the cycle, these vacuoles are quite large, present in all cells and located under the nuclei. On the 17th day, the nuclei, pushed aside by vacuoles, are located in the central part of the cell. On the 18th day, vacuoles appear in the apical part, and nuclei in the basal part of the cells, glycogen begins to be released into the lumen of the glands by apocrine secretion. Best conditions for implantation they are created on the 6-7th day after ovulation, i.e. on the 20-21st day of the cycle, when the secretory activity of the glands is maximum.
On the 21st day of the cycle, the decidual reaction of the endometrial stroma begins. The spiral arteries are sharply tortuous; later, due to a decrease in stromal edema, they are clearly visible. First, decidual cells appear, which gradually form clusters. On the 24th day of the cycle, these accumulations form perivascular eosinophilic couplings. On the 25th day, islands of decidual cells are formed. By the 26th day of the cycle, the decidual reaction becomes the number of neutrophils that migrate there from the blood. Neutrophil infiltration is replaced by necrosis of the functional layer of the endometrium.
Menstruation:
If implantation does not occur, the glands stop producing secretions, and degenerative changes begin in the functional layer of the endometrium. The immediate cause of its rejection is a sharp decrease in the content of estradiol and progesterone as a result of involution of the corpus luteum. In the endometrium, venous outflow decreases and vasodilation occurs. Next, narrowing of the arteries occurs, which leads to ischemia and tissue damage and functional loss of the endometrium. Then bleeding occurs from the fragments of arterioles remaining in the basal layer of the endometrium. Menstruation stops when the arteries narrow, and the endometrium is restored. Thus, the cessation of bleeding in the endometrial vessels differs from hemostasis in other parts of the body.
Typically, bleeding stops as a result of platelet accumulation and fibrin deposition, leading to scarring. In the endometrium, scarring can lead to loss of functional activity (Asherman's syndrome). To avoid these consequences, an alternative hemostasis system is necessary. Vascular contraction is a mechanism to stop bleeding in the endometrium. In this case, scarring is minimized by fibrinolysis, which breaks down blood clots. Later, restoration of the endometrium and the formation of new blood vessels (angiogenesis) leads to the completion of bleeding within 5-7 days from the start of the menstrual cycle.
The effects of estrogen and progesterone withdrawal on menstruation are well established, but the role of paracrine mediators remains unclear. Vasoconstrictors: prostaglandin F2a, endothelium-1 and platelet-activating factor (PAF) can be produced within the endometrium and participate in vascular contraction. They also contribute to the onset of menstruation and further control over it. These mediators can be regulated by the action of vasodilators such as prostaglandin E2, prostacyclin, nitric oxide, which are produced by the endometrium. Prostaglandin F2a has a pronounced vasoconstrictor effect, increases arterial spasm and endometrial ischemia, causes myometrial contractions, which, on the one hand, reduces blood flow, and on the other, promotes the removal of rejected endometrium.
Endometrial repair includes glandular and stromal regeneration and angiogenesis. Vascular endothelial growth factor (VEGF) and fibroplastic growth factor (FGF) are found in the endometrium and are strong angiogenic agents. It was revealed that estrogen-produced glandular and stromal regeneration is enhanced under the influence of epidermal growth factors (EGF). Growth factors such as transforming growth factor (TGF) and interleukins, especially interleukin-1 (IL-1), are of great importance.
Brief overview of the processes occurring in the endometrium
Menstruation:
The main role at the beginning of menstruation is played by arteriolar spasm.
The functional layer of the endometrium (the upper one, making up 75% of the thickness) is rejected.
Menstruation stops due to vasospasm and restoration of the endometrium. Fibrinolysis prevents the formation of adhesions.
Proliferative phase:
Characterized by estrogen-induced proliferation of glands and stroma.
Secretory phase:
Characterized by progesterone-induced glandular secretion.
During the late secretory phase, decidualization is induced.
Decidualization is an irreversible process. In the absence of pregnancy, apoptosis occurs in the endometrium, followed by the appearance of menstruation.
So, the reproductive system is a supersystem, the functional state of which is determined by the reverse afferentation of its constituent subsystems. There are: a long feedback loop between ovarian hormones and the nuclei of the hypothalamus; between ovarian hormones and pituitary gland; a short loop between the anterior pituitary gland and the hypothalamus; ultrashort between RG-LH and neurocytes (nerve cells) of the hypothalamus.
Feedback in a mature woman has both negative and positive character. An example of a negative relationship is the increased release of LH by the anterior pituitary gland in response to low estradiol levels during the early follicular phase of the cycle. An example of positive feedback is the release of LH and FSH in response to the ovulatory maximum of estradiol in the blood. According to the negative feedback mechanism, the formation of RH-LH increases with a decrease in the level of LH in the cells of the anterior pituitary gland.
Summary
GnRH is synthesized by neurons of the infundibulum nucleus, then enters the portal system of the pituitary gland and enters the adenohypophysis through it. GnRH secretion occurs impulsively.
The early stage of development of a group of primordial follicles does not depend on FSH.
As the corpus luteum involutes, the secretion of progesterone and inhibin decreases and the level of FSH increases.
FSH stimulates the growth and development of a group of primordial follicles and their secretion of estrogens.
Estrogens prepare the uterus for implantation by stimulating the proliferation and differentiation of the functional layer of the endometrium and, together with FSH, promote the development of follicles.
According to the two-cell theory of sex hormone synthesis, LH stimulates the synthesis of androgens in thekocytes, which are then, under the influence of FSH, converted into estrogens in granulosa cells.
Increase in estradiol concentration by a negative feedback mechanism, loop
which closes in the pituitary gland and hypothalamus, suppresses the secretion of FSH.
The follicle that will ovulate in a given menstrual cycle is called dominant. Unlike other follicles that have begun to grow, it carries a larger number of FSH receptors and synthesizes a larger amount of estrogens. This allows it to develop, despite the decrease in FSH levels.
Sufficient estrogen stimulation ensures an ovulatory LH peak. It, in turn, causes ovulation, the formation of the corpus luteum and the secretion of progesterone.
The functioning of the corpus luteum depends on the level of LH. When it decreases, the corpus luteum undergoes involution. This usually occurs 12-16 days after ovulation.
If fertilization has occurred, the existence of the corpus luteum is supported by human chorionic gonadotropin. The corpus luteum continues to secrete progesterone, which is necessary to maintain pregnancy in the early stages.
Changes in the female reproductive organs with subsequent bloody discharge from the vagina - this is the menstrual cycle. Levels of regulation of the menstrual cycle can manifest themselves in different women varies, as it depends on the individuality of the organism.
The menstrual cycle is not established immediately, but gradually, it occurs throughout the entire reproductive period of a woman’s life. In most cases, the reproductive period begins at 12–13 years and ends at 45–50 years. As for the duration of the cycle, it ranges from 21 to 35 days. The duration of menstruation itself is from three to seven days. Blood loss during menstruation is about 50–150 ml.
To this day, the cerebral cortex has not yet been fully studied. But the fact has been noticed and confirmed that mental and emotional experiences have a strong impact on the regularity of menstruation. Stress can cause both bleeding itself, which appears out of schedule, and a delay. However, there are cases when women injured after an accident are in a prolonged coma, and the regularity of the cycle is not disrupted. That is, everything depends on the individuality of the organism.
Today, according to the results of many studies, experts can claim that the regulation of the cycle is divided into five levels:
Level 1
The regulation of the cycle is represented by the cerebral cortex. It regulates not only secretions, but also all processes in general. With the help of information coming from the outside world, it is determined emotional condition. And also any changes in the situation are closely related to the woman’s state of mind.
The origin of severe chronic stress greatly influences the occurrence of ovulation and its period. With the negative impact of external factors, changes occur in the menstrual cycle. An example is amenorrhea, which often occurs in women during wartime.
Level 2
The hypothalamus is involved in the second level of regulation. The hypothalamus is a collection of sensitive cells that produce hormones (liberin, as well as releasing factor). They have an effect on the production of another type of hormones, but this time by the adenohypophysis. It is located in the anterior part of the pituitary gland.
The activation or inhibition of the production of neurosecretions and other hormones is greatly influenced by:
- neurotransmitters;
- endorphins;
- dopamine;
- serotonin;
- norepinephrine.
![]()
In the area of the hypothalamus, active production of vasopressin, oxytocin and antidiuretic hormone occurs. They are produced by the posterior lobe of the pituitary gland, called the neurohypophysis.
Level 3
Cells of the anterior pituitary gland actively participate in the third level of regulation. The tissues of the pituitary gland produce a certain amount of gonadotropic hormones. They stimulate proper hormonal functioning of the ovaries. Hormonal regulation of the menstrual cycle is a rather complex process. It involves:
- luteotropic hormones (responsible for activating mammary gland growth, as well as lactation);
- luteinizing hormones (stimulate the development of mature follicles and eggs);
- hormones that stimulate follicle development (with their help the follicle grows and matures).

The adenohypophysis is responsible for the production of gonadotropic hormonal substances. These same hormones are responsible for the proper functioning of the genital organs.
Level 4
The ovaries and their work belong to the fourth level of regulation. As you know, a mature egg matures and is released in the ovaries (during ovulation). And the production of sex hormones also occurs.
Due to the action of follicle-stimulating hormones, the main follicle develops in the ovaries with the subsequent release of the egg. FSH is able to stimulate the production of estrogen, which is responsible for processes in the uterus, as well as for the proper functioning of the vagina and mammary glands.

During the ovulation process, luteinizing and follicle-stimulating hormones take part for the effective production of progesterone (this hormone affects the efficiency of the corpus luteum).
Emerging processes in the ovaries occur cyclically. Their regulation occurs in the form of connections (direct and inverse) with the hypothalamus and pituitary gland. For example, if the level of FSH is elevated, then maturation and growth of the follicle occurs. This increases the concentration of estrogen.
When progesterone accumulates, LH production decreases. The production of female sex hormones by the pituitary gland and hypothalamus activates the processes occurring in the uterus.

Level 5
The fifth level of regulation of the menstrual cycle is the last level where the fallopian tubes, the uterus itself, its tubes and vaginal tissues are involved. Peculiar changes occur in the uterus due to hormonal influences. Modifications occur in the endometrium itself, but everything depends on the phase of the menstrual cycle. According to the results of many studies, four stages of the cycle are distinguished:
- desquamation;
- regeneration;
- proliferation;
- secretion.

If a woman is of reproductive age, then her periods should occur regularly. Menstruation, under normal conditions, should be profuse, painless or with little discomfort. As for the duration in a 28-day cycle, it is 3-5 days.
Phases of the menstrual cycle
When studying the female body, it has been proven that it contains a certain amount of female and male hormones. They are called androgens. Women's sex hormones are more involved in the regulation of the menstrual cycle. Each menstrual cycle is the body’s preparation for a future pregnancy.
There are a certain number of phases in a woman's menstrual cycle:
First phase
The first phase is the follicular phase. During its manifestation, the development of the egg occurs, while the old endometrial layer is rejected - this is how menstruation begins. When the uterus contracts, pain symptoms appear in the lower abdomen.
Depending on the characteristics of the body, some women have a menstrual cycle of two days, while others have as many as seven. During the first half of the cycle, a follicle develops in the ovaries; over time, an egg ready for fertilization will be released. This process is called ovulation. The phase in question lasts from 7 to 22 days. It depends on the body.

In the first phase, ovulation most often occurs from days 7 to 21 of the cycle. The maturation of the egg occurs on the 14th day. Next, the egg moves to the uterine tubes.
Second phase
The appearance of the corpus luteum occurs during the second phase, just in the post-ovulation period. A follicle that has burst is transformed into a corpus luteum, which begins to produce hormones, including progesterone. He is responsible for pregnancy and its support.

During the second phase, the endometrium thickens in the uterus. This is how preparation occurs for the reception of a fertilized egg. The top layer is enriched with nutrients. Typically, this phase lasts approximately 14 days (the first day after ovulation is considered). If fertilization does not occur, then discharge appears - menstruation. So the prepared endometrium comes out.
In most cases, the menstrual cycle begins on the first day of discharge. For this reason, the menstrual cycle is counted from the first day of discharge to the first day of subsequent periods. Under normal conditions, the menstrual cycle pattern can vary from 21 to 34 days.
When an egg and a sperm meet, fertilization occurs. Next, the egg moves closer to the wall of the uterus, where there is a thick layer of the endometrium, and attaches to it (ingrown). The fertilized egg is born. After this, the female body is reconstructed and begins to produce hormones in large quantities, which should participate in a kind of “switching off” of the menstrual cycle throughout the entire pregnancy.

With the help of natural hormonal intervention, the expectant mother's body prepares for the upcoming birth.
Causes of irregular menstrual cycle
The reasons that cause menstruation irregularities in women are very diverse:
- after treatment with hormonal drugs;
- complications after diseases of the genital organs (ovarian tumor, uterine fibroids, endometriosis);
- consequences of diabetes;
- consequences after abortions and spontaneous miscarriages;
- consequences of chronic and acute general infectious pathologies, including infections that are transmitted through sexual intercourse;

- inflammation of the pelvic organs (endometritis, salpingoophoritis);
- at incorrect location spirals inside the uterus;
- complications after concomitant endocrine diseases associated with the thyroid gland and adrenal glands;
- the occurrence of frequent stressful situations, mental trauma, poor nutrition;
- disorders inside the ovary (they can be congenital or acquired).

Violations are different, it all depends on the individuality of the body and its characteristics.
The connection between menstruation and ovulation
The inner walls of the uterus are covered with a special layer of cells, their totality is called the endometrium. During the first half of the cycle, before ovulation occurs, endometrial cells grow, divide, and proliferate. And by half the cycle the endometrial layer becomes thick. The walls of the uterus prepare to receive a fertilized egg.

During ovulation, cells change their functionality due to the action of progesterone. The process of cell division stops and is replaced by the release of a special secretion that facilitates the ingrowth of a fertilized egg - a zygote.
If fertilization has not occurred, and the endometrium is highly developed, then large doses of progesterone are required. If the cells do not receive it, then vasoconstriction begins. When tissue nutrition deteriorates, they die. Towards the end of the cycle, day 28, the vessels burst and blood appears. With its help, the endometrium is washed out of the uterine cavity.
After 5–7 days, the burst vessels are restored and fresh endometrium appears. Menstrual flow decreases and stops. Everything repeats itself - this is the beginning of the next cycle.

Amenorrhea and its manifestations
Amenorrhea can manifest itself as the absence of menstruation for six months, or even more. There are two types of amenorrhea:
- false (most cyclic changes in the reproductive system occur, but there is no bleeding);
- true (accompanied by the absence of cyclic changes not only in the female reproductive system, but also in her body as a whole).

With false amenorrhea, the outflow of blood is disrupted, in this case atresia may appear in different stages. A complication may be the occurrence of more complex diseases.
True amenorrhea occurs:
- pathological;
- physiological.

With primary pathological amenorrhea, there may be no signs of menstruation even at 16 or 17 years of age. In case of secondary pathology, menstruation ceases in women for whom everything was fine.
Signs of physiological amenorrhea are observed in girls. When there is no activity of the pituitary-hypothalamus systemic ligament. But physical amenorrhea is also observed during pregnancy.
Changes in the female reproductive organs with subsequent bloody discharge from the vagina - this is the menstrual cycle. The levels of regulation of the menstrual cycle can manifest themselves differently in different women, as it depends on the individuality of the body.
The menstrual cycle is not established immediately, but gradually, it occurs throughout the entire reproductive period of a woman’s life. In most cases, the reproductive period begins at 12–13 years and ends at 45–50 years. As for the duration of the cycle, it ranges from 21 to 35 days. The duration of menstruation itself is from three to seven days. Blood loss during menstruation is about 50–150 ml.
To this day, the cerebral cortex has not yet been fully studied. But the fact has been noticed and confirmed that mental and emotional experiences have a strong impact on the regularity of menstruation. Stress can cause both bleeding itself, which appears out of schedule, and a delay. However, there are cases when women injured after an accident are in a prolonged coma, and the regularity of the cycle is not disrupted. That is, everything depends on the individuality of the organism.
Today, according to the results of many studies, experts can claim that the regulation of the cycle is divided into five levels:
Level 1
The regulation of the cycle is represented by the cerebral cortex. It regulates not only secretions, but also all processes in general. With the help of information coming from the outside world, the emotional state is determined. And also any changes in the situation are closely related to the woman’s state of mind.
The origin of severe chronic stress greatly influences the occurrence of ovulation and its period. With the negative impact of external factors, changes occur in the menstrual cycle. An example is amenorrhea, which often occurs in women during wartime.
Level 2
The hypothalamus is involved in the second level of regulation. The hypothalamus is a collection of sensitive cells that produce hormones (liberin, as well as releasing factor). They have an effect on the production of another type of hormones, but this time by the adenohypophysis. It is located in the anterior part of the pituitary gland.
The activation or inhibition of the production of neurosecretions and other hormones is greatly influenced by:
- neurotransmitters;
- endorphins;
- dopamine;
- serotonin;
- norepinephrine.
![]()
In the area of the hypothalamus, active production of vasopressin, oxytocin and antidiuretic hormone occurs. They are produced by the posterior lobe of the pituitary gland, called the neurohypophysis.
Level 3
Cells of the anterior pituitary gland actively participate in the third level of regulation. The tissues of the pituitary gland produce a certain amount of gonadotropic hormones. They stimulate proper hormonal functioning of the ovaries. Hormonal regulation of the menstrual cycle is a rather complex process. It involves:
- luteotropic hormones (responsible for activating mammary gland growth, as well as lactation);
- luteinizing hormones (stimulate the development of mature follicles and eggs);
- hormones that stimulate follicle development (with their help the follicle grows and matures).

The adenohypophysis is responsible for the production of gonadotropic hormonal substances. These same hormones are responsible for the proper functioning of the genital organs.
Level 4
The ovaries and their work belong to the fourth level of regulation. As you know, a mature egg matures and is released in the ovaries (during ovulation). And the production of sex hormones also occurs.
Due to the action of follicle-stimulating hormones, the main follicle develops in the ovaries with the subsequent release of the egg. FSH is able to stimulate the production of estrogen, which is responsible for processes in the uterus, as well as for the proper functioning of the vagina and mammary glands.

During the ovulation process, luteinizing and follicle-stimulating hormones take part for the effective production of progesterone (this hormone affects the efficiency of the corpus luteum).
Emerging processes in the ovaries occur cyclically. Their regulation occurs in the form of connections (direct and inverse) with the hypothalamus and pituitary gland. For example, if the level of FSH is elevated, then maturation and growth of the follicle occurs. This increases the concentration of estrogen.
When progesterone accumulates, LH production decreases. The production of female sex hormones by the pituitary gland and hypothalamus activates the processes occurring in the uterus.

Level 5
The fifth level of regulation of the menstrual cycle is the last level where the fallopian tubes, the uterus itself, its tubes and vaginal tissues are involved. Peculiar changes occur in the uterus due to hormonal influences. Modifications occur in the endometrium itself, but everything depends on the phase of the menstrual cycle. According to the results of many studies, four stages of the cycle are distinguished:
- desquamation;
- regeneration;
- proliferation;
- secretion.

If a woman is of reproductive age, then her periods should occur regularly. Menstruation, under normal conditions, should be profuse, painless or with little discomfort. As for the duration in a 28-day cycle, it is 3-5 days.
Phases of the menstrual cycle
When studying the female body, it has been proven that it contains a certain amount of female and male hormones. They are called androgens. Women's sex hormones are more involved in the regulation of the menstrual cycle. Each menstrual cycle is the body’s preparation for a future pregnancy.
There are a certain number of phases in a woman's menstrual cycle:
First phase
The first phase is the follicular phase. During its manifestation, the development of the egg occurs, while the old endometrial layer is rejected - this is how menstruation begins. When the uterus contracts, pain symptoms appear in the lower abdomen.
Depending on the characteristics of the body, some women have a menstrual cycle of two days, while others have as many as seven. During the first half of the cycle, a follicle develops in the ovaries; over time, an egg ready for fertilization will be released. This process is called ovulation. The phase in question lasts from 7 to 22 days. It depends on the body.

In the first phase, ovulation most often occurs from days 7 to 21 of the cycle. The maturation of the egg occurs on the 14th day. Next, the egg moves to the uterine tubes.
Second phase
The appearance of the corpus luteum occurs during the second phase, just in the post-ovulation period. A follicle that has burst is transformed into a corpus luteum, which begins to produce hormones, including progesterone. He is responsible for pregnancy and its support.

During the second phase, the endometrium thickens in the uterus. This is how preparation occurs for the reception of a fertilized egg. The top layer is enriched with nutrients. Typically, this phase lasts approximately 14 days (the first day after ovulation is considered). If fertilization does not occur, then discharge appears - menstruation. So the prepared endometrium comes out.
In most cases, the menstrual cycle begins on the first day of discharge. For this reason, the menstrual cycle is counted from the first day of discharge to the first day of subsequent periods. Under normal conditions, the menstrual cycle pattern can vary from 21 to 34 days.
When an egg and a sperm meet, fertilization occurs. Next, the egg moves closer to the wall of the uterus, where there is a thick layer of the endometrium, and attaches to it (ingrown). The fertilized egg is born. After this, the female body is reconstructed and begins to produce hormones in large quantities, which should participate in a kind of “switching off” of the menstrual cycle throughout the entire pregnancy.

With the help of natural hormonal intervention, the expectant mother's body prepares for the upcoming birth.
Causes of irregular menstrual cycle
The reasons that cause menstruation irregularities in women are very diverse:
- after treatment with hormonal drugs;
- complications after diseases of the genital organs (ovarian tumor, uterine fibroids, endometriosis);
- consequences of diabetes;
- consequences after abortions and spontaneous miscarriages;
- consequences of chronic and acute general infectious pathologies, including infections that are transmitted through sexual intercourse;

- inflammation of the pelvic organs (endometritis, salpingoophoritis);
- if the IUD is incorrectly positioned inside the uterus;
- complications after concomitant endocrine diseases associated with the thyroid gland and adrenal glands;
- the occurrence of frequent stressful situations, mental trauma, poor nutrition;
- disorders inside the ovary (they can be congenital or acquired).

Violations are different, it all depends on the individuality of the body and its characteristics.
The connection between menstruation and ovulation
The inner walls of the uterus are covered with a special layer of cells, their totality is called the endometrium. During the first half of the cycle, before ovulation occurs, endometrial cells grow, divide, and proliferate. And by half the cycle the endometrial layer becomes thick. The walls of the uterus prepare to receive a fertilized egg.

During ovulation, cells change their functionality due to the action of progesterone. The process of cell division stops and is replaced by the release of a special secretion that facilitates the ingrowth of a fertilized egg - a zygote.
If fertilization has not occurred, and the endometrium is highly developed, then large doses of progesterone are required. If the cells do not receive it, then vasoconstriction begins. When tissue nutrition deteriorates, they die. Towards the end of the cycle, day 28, the vessels burst and blood appears. With its help, the endometrium is washed out of the uterine cavity.
After 5–7 days, the burst vessels are restored and fresh endometrium appears. Menstrual flow decreases and stops. Everything repeats itself - this is the beginning of the next cycle.

Amenorrhea and its manifestations
Amenorrhea can manifest itself as the absence of menstruation for six months, or even more. There are two types of amenorrhea:
- false (most cyclic changes in the reproductive system occur, but there is no bleeding);
- true (accompanied by the absence of cyclic changes not only in the female reproductive system, but also in her body as a whole).

With false amenorrhea, the outflow of blood is disrupted, in this case atresia may appear in different stages. A complication may be the occurrence of more complex diseases.
True amenorrhea occurs:
- pathological;
- physiological.
With primary pathological amenorrhea, there may be no signs of menstruation even at 16 or 17 years of age. In case of secondary pathology, menstruation ceases in women for whom everything was fine.
Signs of physiological amenorrhea are observed in girls. When there is no activity of the pituitary-hypothalamus systemic ligament. But physical amenorrhea is also observed during pregnancy.
Menstrual cycle is a complex of complex biological processes occurring in a woman’s body, which is characterized by cyclical changes in all parts of the reproductive system and is intended to ensure conception and development of pregnancy.
Menstruation - cyclical short-term uterine bleeding, resulting from the rejection of the functional layer of the endometrium at the end of the two-phase menstrual cycle. The first day of menstruation is considered the first day of the menstrual cycle.
The duration of the menstrual cycle is the time between the first days of the last two menstruation and normally ranges from 21 to 36 days, with an average of 28 days; duration of menstruation - from 2 to 7 days; volume of blood loss - 40-150 ml.
Physiology of the female reproductive system
Neurohumoral regulation of the reproductive system is organized according to a hierarchical principle. It is distinguished
five levels, each of which is regulated by overlying structures via a feedback mechanism: cerebral cortex, hypothalamus, pituitary gland, ovaries, uterus and other target tissues for sex hormones.
Cortex
The highest level of regulation is the cerebral cortex: specialized neurons receive information about the state of the internal and external environment, convert it into neurohumoral signals, which enter the neurosensory cells of the hypothalamus through the system of neurotransmitters. The function of neurotransmitters is performed by biogenic amines-catecholamines - dopamine and norepinephrine, indoles - serotonin, as well as opioid neuropeptides - endorphins and enkephalins.
Dopamine, norepinephrine and serotonin control hypothalamic neurons secreting gonadotropin-releasing hormone (GnRH): dopamine supports the secretion of GnRH in the arcuate nuclei, and also inhibits the release of prolactin by the adenohypophysis; norepinephrine regulates the transmission of impulses to the prebiotic nuclei of the hypothalamus and stimulates the ovulatory release of GnRH; serotonin controls the cyclic secretion of luteinizing hormone (LH). Opioid peptides suppress LH secretion, inhibit the stimulating effect of dopamine, and their antagonist, naloxone, causes a sharp rise in GnRH levels.
Hypothalamus
The hypothalamus is one of the main brain structures involved in the regulation of autonomic, visceral, trophic and neuroendocrine functions. The nuclei of the pituitary zone of the hypothalamus (supraoptic, paraventricular, arcuate and ventromedial) produce specific neurosecretes with diametrically opposite pharmacological effects: releasing hormones, releasing tropic hormones in the anterior lobe of the pituitary gland and statins, inhibiting their release.
Currently, 6 releasing hormones (RG) are known: gonadotropic RG, thyroid-stimulating RG, adrenocorticotropic RG, somatotropic RG, melanotropic RG, prolactin-RG and three statins: melanotropic inhibitory hormone, somatotropic
prolactin-inhibiting hormone, prolactin-inhibiting hormone.
GnRH is released into the portal bloodstream in a pulsating manner: once every 60-90 minutes. This rhythm is called circhoral. The frequency of GnRH release is genetically programmed. During the menstrual cycle, it changes within small limits: the maximum frequency is recorded in the preovulatory period, the minimum in phase II of the cycle.
Pituitary
Basophilic cells of the adenohypophysis (gonadotropocytes) secrete hormones - gonadotropins, which are directly involved in the regulation of the menstrual cycle; these include: follitropin, or follicle-stimulating hormone (FSH) and lutropin, or luteinizing hormone (LH); a group of acidophilic cells of the anterior pituitary gland - lactotropocytes - produce prolactin (PRL).
The secretion of prolactin has circadian rhythm discharge.
There are two types of gonadotropin secretion - tonic and cyclic. Tonic release of gonadotropins promotes the development of follicles and their production of estrogens; cyclical - ensures a change in phases of low and high secretion of hormones and, in particular, their preovulatory peak.
Biological effect of FSH: stimulates the growth and maturation of follicles, proliferation of granulosa cells; induces the formation of LH receptors on the surface of granulosa cells; increases the level of aromatase in the ripening follicle.
Biological action of LH: stimulates the synthesis of androgens (estrogens precursors) in theca cells; activates the action of prostaglandins and proteolytic enzymes, which lead to thinning and rupture of the follicle; luteinization of granulosa cells occurs (formation of the corpus luteum); together with PRL, it stimulates the synthesis of progesterone in luteinized granulosa cells of the ovulated follicle.
Biological effects of PRL: stimulates the growth of mammary glands and regulates lactation; has a fat-mobilizing and hypotensive effect; in increased quantities inhibits the growth and maturation of the follicle; participates in the regulation of the endocrine function of the corpus luteum.
Ovaries
The generative function of the ovaries is characterized by cyclic maturation of the follicle, ovulation, release of an egg capable of conception, and provision of secretory transformations in the endometrium necessary for the reception of a fertilized egg.
The main morphofunctional unit of the ovaries is the follicle. In accordance with the International Histological Classification (1994), 4 types of follicles are distinguished: primordial, primary, secondary (antral, cavitary, vesicular), mature (preovulatory, graafian).
Primordial follicles are formed in the fifth month of intrauterine development of the fetus (as a result of meiosis, they contain a haploid set of chromosomes) and continue to exist throughout the woman’s life until the onset of menopause and for several years after the permanent cessation of menstruation. By the time of birth, both ovaries contain about 300-500 thousand primordial follicles, later their number sharply decreases and by the age of 40 it is about 40-50 thousand due to physiological atresia.
The primordial follicle consists of an egg surrounded by a single row of follicular epithelium; its diameter does not exceed 50 microns.
The stage of the primary follicle is characterized by increased proliferation of the follicular epithelium, the cells of which acquire a granular structure and form a granular (granulosa) layer. The secretion secreted by the cells of this layer accumulates in the intercellular space. The size of the egg gradually increases to 55-90 microns in diameter.
During the formation of the secondary follicle, its walls are stretched by the liquid: the oocyte in this follicle no longer increases (to at this moment its diameter is 100-180 microns), but the diameter of the follicle itself increases and amounts to 20-24 mm.
In a mature follicle, the egg, enclosed in the oviductal tubercle, is covered with a transparent membrane, on which granular cells are located in a radial direction and form a corona radiata.
Ovulation is the rupture of a mature follicle with the release of an egg cell, surrounded by the corona radiata, into the abdominal cavity,
and then into the ampulla of the fallopian tube. Violation of the integrity of the follicle occurs in its most convex and thinnest part, called the stigma.
In a healthy woman, one follicle matures during the menstrual cycle, and about 400 eggs ovulate during the entire reproductive period; the remaining oocytes undergo atresia. The viability of the egg remains for 12-24 hours.
Luteinization is a specific transformation of the follicle in the postovulatory period. As a result of luteinization (coloring yellow due to the accumulation of lipochrome pigment - lutein), reproduction and proliferation of cells of the granular membrane of the ovulated follicle, a formation called the corpus luteum is formed. In cases where fertilization does not occur, the corpus luteum exists for 12-14 days and then undergoes reverse development.
Thus, the ovarian cycle consists of two phases - follicular and luteal. The follicular phase begins after menstruation and ends with ovulation; The luteal phase occupies the period between ovulation and the onset of menstruation.
Hormonal function of the ovaries
During their existence, the cells of the granulosa membrane, the inner shell of the follicle and the corpus luteum perform the function of an endocrine gland and synthesize three main types of steroid hormones - estrogens, gestagens, and androgens.
Estrogens are secreted by cells of the granular membrane, the inner membrane and, to a lesser extent, by interstitial cells. Estrogens are formed in small quantities in the corpus luteum, the adrenal cortex, and in pregnant women - in the placenta. The main estrogens of the ovary are estradiol, estrone and estriol (the first two hormones are predominantly synthesized). The activity of 0.1 mg of estrone is taken as 1 IU of estrogenic activity. According to the Allen and Doisy test (the smallest amount of the drug that causes estrus in castrated mice), estradiol has the greatest activity, followed by estrone and estriol (ratio 1: 7: 100).
Metabolism of estrogen. Estrogens circulate in the blood in free and protein-bound (biologically inactive) form. From the blood, estrogens enter the liver, where they are inactivated by forming paired compounds with sulfuric and glucuronic acids, which enter the kidneys and are excreted in the urine.
The effect of estrogen on the body is realized as follows:
Vegetative effect (strictly specific) - estrogens have a specific effect on the female genital organs: stimulate the development of secondary sexual characteristics, cause hyperplasia and hypertrophy of the endometrium and myometrium, improve blood supply to the uterus, promote the development of the excretory system of the mammary glands;
- generative effect (less specific) - estrogens stimulate trophic processes during follicle maturation, promote the formation and growth of granulosa, egg formation and development of the corpus luteum - prepare the ovary for the effects of gonadotropic hormones;
- general effect (non-specific) - estrogens in physiological quantities stimulate the reticuloendothelial system (increase the production of antibodies and the activity of phagocytes, increasing the body’s resistance to infections), retain nitrogen, sodium, fluid in soft tissues, calcium, phosphorus in bones. Cause an increase in the concentration of glycogen, glucose, phosphorus, creatinine, iron and copper in the blood and muscles; reduce cholesterol, phospholipids and total fat in the liver and blood, accelerate the synthesis of higher fatty acids.
Progestins are secreted by luteal cells of the corpus luteum, luteinizing granulosa cells and follicular membranes, as well as the adrenal cortex and placenta. The main gestagen of the ovaries is progesterone. In addition to progesterone, the ovaries synthesize 17a-hydroxyprogesterone, D4-pregnenol-20a-OH-3, D4-pregnenol-20b-OH-3.
Effects of gestagens:
Autonomic effects - gestagens have an effect on the genitals after preliminary estrogen stimulation: they suppress the proliferation of the endometrium caused by estrogens, carry out secretory transformations in the endometrium; during fertilization of the egg, gestagens suppress ovulation, prevent uterine contractions (“protector” of pregnancy), and promote the development of alveoli in the mammary glands;
- generative effect - gestagens in small doses stimulate the secretion of FSH, in large doses they block both FSH and LH; cause excitation of the thermoregulatory center located in the hypothalamus, which is manifested by an increase in basal temperature;
- general effect - gestagens under physiological conditions reduce the content of amine nitrogen in the blood plasma, increase the excretion of amino acids, increase the secretion of gastric juice, and inhibit the secretion of bile.
Androgens are secreted by cells of the inner lining of the follicle, interstitial cells (in small quantities) and cells of the zona reticularis of the adrenal cortex (the main source). The main androgens of the ovaries are androstenedione and dehydroepiandrosterone; testosterone and epitestosterone are synthesized in small doses.
The specific effect of androgens on the reproductive system depends on the level of their secretion (small doses stimulate the function of the pituitary gland, large doses block it) and can manifest itself in the form of the following effects:
Virile effect - large doses of androgens cause clitoral hypertrophy, male-type hair growth, growth of the cricoid cartilage, and the appearance of acne;
- gonadotropic effect - small doses of androgens stimulate the secretion of gonadotropic hormones, promote the growth and maturation of the follicle, ovulation, luteinization;
- antigonadotropic effect - high level the concentration of androgens in the preovulatory period suppresses ovulation and subsequently causes follicular atresia;
- estrogenic effect - in small doses androgens cause proliferation of the endometrium and vaginal epithelium;
- antiestrogenic effect - large doses of androgens block proliferation processes in the endometrium and lead to the disappearance of acidophilic cells in the vaginal smear.
- general effect - androgens have pronounced anabolic activity, enhance protein synthesis by tissues; retain nitrogen, sodium and chlorine in the body, reduce the excretion of urea. Accelerate bone growth and ossification of epiphyseal cartilage, increase the number of red blood cells and hemoglobin.
Other ovarian hormones: inhibin, synthesized by granular cells, has an inhibitory effect on the synthesis of FSH; oxytocin (found in follicular fluid, corpus luteum) - in the ovaries it has a luteolytic effect, promotes regression of the corpus luteum; relaxin, formed in granulosa cells and the corpus luteum, promotes ovulation, relaxes the myometrium.
Uterus
Under the influence of ovarian hormones, cyclic changes are observed in the myometrium and endometrium, corresponding to the follicular and luteal phases in the ovaries. The follicular phase is characterized by hypertrophy of the cells of the muscular layer of the uterus, and the luteal phase is characterized by their hyperplasia. Functional changes in the endometrium are reflected by a sequential change in the stages of regeneration, proliferation, secretion, and desquamation (menstruation).
The regeneration phase (3-4 days of the menstrual cycle) is short, characterized by the regeneration of the endometrium from basal milk cells.
Epithelization of the wound surface occurs from the marginal sections of the glands of the basal layer, as well as from the non-rejected deep sections of the functional layer.
The proliferation phase (corresponding to the follicular phase) is characterized by transformations that occur under the influence of estrogens.
Early stage of proliferation (before 7-8 days of the menstrual cycle): the surface of the mucous membrane is lined with flattened cylindrical epithelium, the glands look like straight or slightly convoluted short tubes with a narrow lumen, the epithelium of the glands is single-row, low, cylindrical.
The middle stage of proliferation (up to 10-12 days of the menstrual cycle): the surface of the mucous membrane is lined with high prismatic epithelium, the glands lengthen, become more convoluted, the stroma is swollen and loosened.
Late stage of proliferation (before ovulation): the glands become sharply tortuous, sometimes spur-shaped, their lumen expands, the epithelium lining the glands is multirowed, the stroma is juicy, spiral arteries reach the surface of the endometrium, moderately tortuous.
The secretion phase (corresponding to the luteal phase) reflects changes due to the effects of progesterone.
The early stage of secretion (before the 18th day of the menstrual cycle) is characterized by further development of the glands and expansion of their lumen, the most characteristic feature This stage is the appearance of subnuclear vacuoles containing glycogen in the epithelium.
The middle stage of secretion (19-23 days of the menstrual cycle) - reflects the transformations characteristic of the heyday of the corpus luteum, i.e. period of maximum gestagenic saturation. The functional layer becomes higher, clearly divided into deep and superficial layers: deep - spongy, spongy; superficial - compact. The glands expand, their walls become folded; in the lumen of the glands a secret appears containing glycogen and acidic mucopolysaccharides. The spiral arteries are sharply tortuous and form “tangles” (the most reliable sign that determines the luteinizing effect). Structure and functional state endometrium on days 20-22 of the 28-day menstrual cycle represent optimal conditions for blastocyst implantation.
Late stage of secretion (24-27 days of the menstrual cycle): processes associated with regression of the corpus luteum and, consequently, a decrease in the concentration of hormones produced by it are observed - endometrial trophism is disrupted, and degenerative changes are formed.
Morphologically, the endometrium regresses, and signs of ischemia appear. At the same time, the juiciness of the tissue decreases, which leads to wrinkling of the stroma of the functional layer. The folding of the walls of the glands intensifies. On the 26-27th day of the menstrual cycle, lacunar expansion of capillaries and focal hemorrhages into the stroma are observed in the superficial zones of the compact layer; due to the melting of the fibrous structures, areas of separation of the cells of the stroma and the epithelium of the glands appear. This state of the endometrium is called “anatomical menstruation” and immediately precedes clinical menstruation.
Bleeding phase, desquamation (28-29 days of the menstrual cycle). In the mechanism of menstrual bleeding, leading importance is given to circulatory disorders caused by prolonged spasm of the arteries (stasis, blood clot formation, fragility and permeability of the vascular wall, hemorrhages into the stroma, leukocyte infiltration). The result of these transformations is necrobiosis of the tissue and its melting. Due to the dilation of blood vessels that occurs after a long spasm, a large amount of blood enters the endometrial tissue, which leads to rupture of blood vessels and rejection - desquamation - of necrotic sections of the functional layer of the endometrium, i.e. to menstrual bleeding.
Target tissues are the points of application of the action of sex hormones. These include: brain tissue, genitals, mammary glands, hair follicles and skin, bones, adipose tissue. The cells of these organs and tissues contain receptors for sex hormones. The mediator of this level of regulation of the reproductive system is cAMP, which regulates metabolism in the cells of target tissues in accordance with the needs of the body in response to the influence of hormones. Intercellular regulators also include prostaglandins, which are formed from unsaturated fatty acids in all tissues of the body. The action of prostaglandins is realized through cAMP.
The brain is the target organ for sex hormones. Sex hormones, through growth factors, can influence both neurons and glial cells. Sex hormones influence the formation of signals in those areas of the central nervous system that are involved in the regulation of reproductive behavior (ventromedial, hypothalamic and amygdala nuclei), as well as in areas that regulate the synthesis and release of hormones by the pituitary gland (in the arcuate hypothalamic nucleus and preoptic region).
In the hypothalamus, the main target for sex hormones are neurons that form the arcuate nucleus, in which GnRH is synthesized, released in a pulsed manner. Opioids can have excitatory and inhibitory effects on GnRH-synthesizing neurons of the hypothalamus. Estrogens stimulate the synthesis of receptors for endogenous opioids. β-endorphin (β-EP) is the most active endogenous opioid peptide that affects behavior, causes analgesia, is involved in thermoregulation and has neuroendocrine properties. In postmenopause and after oophorectomy, the level of r-EP decreases, which contributes to the occurrence of hot flashes and increased sweating, as well as changes in mood, behavior, and monoceptive disorders. Estrogens excite the central nervous system by increasing the sensitivity of neurotransmitter receptors in estrogen-sensitive neurons, leading to mood elevation, increased activity, and antidepressant effects. Low levels of estrogen during menopause cause the development of depression.
Androgens also play a role in women's sexual behavior, emotional reactions and cognitive function. Androgen deficiency during menopause leads to decreased pubic hair, muscle strength, and decreased libido.
The fallopian tubes
The functional state of the fallopian tubes varies depending on the phase of the menstrual cycle. Thus, in the luteal phase of the cycle, the ciliated apparatus of the ciliated epithelium is activated, the height of its cells increases, over the apical part of which secretions accumulate. The tone of the muscular layer of the tubes also changes: by the time of ovulation, a decrease and intensification of their contractions are recorded, which have both a pendulum and rotational-translational character. Muscle activity is unequal in different parts of the organ: peristaltic waves are more characteristic of distal sections. Activation of the ciliated apparatus of the ciliated epithelium, lability of the muscle tone of the fallopian tubes in the luteal phase, asynchronism and diversity of contractile activity in different parts of the organ are collectively determined to ensure optimal conditions for gamete transport.
In addition, during different phases of the menstrual cycle, the nature of microcirculation in the vessels of the fallopian tubes changes. During the period of ovulation, the veins that encircle the infundibulum in a ring and penetrate deep into its fimbriae become filled with blood, as a result of which the tone of the fimbriae increases and the infundibulum, approaching the ovary, covers it, which, in parallel with other mechanisms, ensures the entry of the ovulated egg into the tube. When the stagnation of blood in the annular veins of the funnel stops, the latter moves away from the surface of the ovary.
Vagina
During the menstrual cycle, the structure of the vaginal epithelium undergoes proliferative and regressive phases. The proliferative phase corresponds to the follicular stage of the ovaries and is characterized by the proliferation, enlargement and differentiation of epithelial cells. During the period corresponding to the early follicular phase, epithelial growth occurs mainly due to the cells of the basal layer; by the middle of the phase, the content of intermediate cells increases. In the preovulatory period, when the vaginal epithelium reaches its maximum thickness - 150-300 microns - activation of the maturation of cells in the superficial layer is observed.
The regressive phase corresponds to the luteal stage. In this phase, the growth of the epithelium stops, its thickness decreases, and some cells undergo reverse development. The phase ends with the desquamation of cells in large and compact groups.
The mammary glands increase during the menstrual cycle, starting from the moment of ovulation and reaching a maximum on the first day of menstruation. Before menstruation, there is an increase in blood flow, an increase in fluid content in the connective tissue, the development of interlobular edema, and expansion of the interlobular ducts, which leads to an enlargement of the mammary gland.
Neurohumoral regulation of the menstrual cycle
Regulation of the normal menstrual cycle is carried out at the level of specialized neurons of the brain, which receive information about the state of the internal and external environment and convert it into neurohormonal signals. The latter enter the neurosecretory cells of the hypothalamus through the neurotransmitter system and stimulate the secretion of GnRH. GnRH, through the local circulatory network of the hypothalamic-pituitary portal system, penetrates directly into the adenohypophysis, where it provides circhoral secretion and release of glycoprotein gonadotropins: FSH and LH. They enter the ovaries through the circulatory system: FSH stimulates the growth and maturation of the follicle, LH stimulates steroidogenesis. Under the influence of FSH and LH, the ovaries produce estrogens and progesterone with the participation of PRL, which, in turn, cause cyclic transformations in target organs: the uterus, fallopian tubes, vagina, as well as in the skin, hair follicles, bones, adipose tissue, brain.
The functional state of the reproductive system is regulated by certain connecting links between its constituent subsystems:
a) a long loop between the ovaries and the nuclei of the hypothalamus;
b) a long loop between ovarian hormones and the pituitary gland;
c) an ultrashort loop between gonadotropin-releasing hormone and hypothalamic neurocytes.
The relationship between these subsystems is based on the principle of feedback, which has both a negative (plus-minus interaction) and positive (plus-plus interaction) character. The harmony of the processes occurring in the reproductive system is determined by: the usefulness of gonadotropic stimulation; normal functioning of the ovaries, especially the correct course of processes in the Graafian vesicle and the corpus luteum that then forms in its place; the correct interaction of the peripheral and central links - reverse afferentation.
The role of prostaglandins in the regulation of the female reproductive system
Prostaglandins represent a special class of biologically active substances (unsaturated hydroxylated fatty acids), which are found in almost all tissues of the body. Prostaglandins are synthesized inside the cell and released in the same cells on which they act. Therefore, prostaglandins are called cellular hormones. The human body does not have a supply of prostaglandins, since they are inactivated within a short period when they enter the bloodstream. Estrogens and oxytocin enhance the synthesis of prostaglandins, progesterone and prolactin have an inhibitory effect. Non-steroidal anti-inflammatory drugs have a powerful anti-prostaglandin effect.
The role of prostaglandins in the regulation of the female reproductive system:
1. Participation in the ovulation process. Under the influence of estrogens, the content of prostaglandins in granulosa cells reaches a maximum at the time of ovulation and ensures rupture of the wall of the mature follicle (prostaglandins increase the contractile activity of the smooth muscle elements of the follicle membrane and reduce the formation of collagen). Prostaglandins are also attributed the ability to luteolysis - regression of the corpus luteum.
2. Transport of the egg. Prostaglandins influence the contractile activity of the fallopian tubes: in the follicular phase they cause contraction of the isthmic section of the tubes, in the luteal phase - its relaxation, increased peristalsis of the ampulla, which promotes the penetration of the egg into the uterine cavity. In addition, prostaglandins act on the myometrium: from the tubal angles towards the fundus of the uterus, the stimulating effect of prostaglandins is replaced by an inhibitory effect and, thus, promotes nidation of the blastocyst.
3. Regulation of menstrual bleeding. The intensity of menstruation is determined not only by the structure of the endometrium at the time of its rejection, but also by the contractile activity of the myometrium, arterioles, and platelet aggregation.
These processes are closely related to the degree of synthesis and degradation of prostaglandins.
Modern teaching about menstrual function.
Regulation of menstrual function.
Gonadotropic and ovarian hormones.
Morphological changes in the ovaries and endometrium.
Ovarian and uterine cycle.
Functional diagnostic tests.
Periods of a woman's life.
The influence of the environment on the development of the female body.
It is more correct to talk not about the menstrual cycle, but about the reproductive system, which, like others, is a functional system (according to Anokhin, 1931), and exhibits functional activity only during childbearing age.
A functional system is an integral formation that includes central and peripheral links and works on the principle of feedback, with reverse afferentation according to the final effect.
All other systems maintain homeostasis, and the reproductive system supports reproduction - the existence of the human race.
The system reaches functional activity by the age of 16-17 years. By the age of 40, reproductive function fades, and by the age of 50, hormonal function fades.
Menstrual cycle is a complex, rhythmically repeating biological process that prepares a woman’s body for pregnancy.
During the menstrual cycle, periodic changes occur in the body associated with ovulation and culminating in bleeding from the uterus. Monthly, cyclically occurring uterine bleeding is called menses(from Latin menstruus - monthly or regulus). The appearance of menstrual bleeding indicates the end of physiological processes that prepare the woman’s body for pregnancy and the death of the egg. Menstruation is the shedding of the functional layer of the uterine lining.
Menstrual function - features of the menstrual cycles during a certain period of a woman’s life.
Cyclic menstrual changes begin in a girl’s body during puberty (from 7-8 to 17-18 years). At this time, the reproductive system matures, the physical development of the female body ends - body growth in length, ossification of the growth zones of tubular bones; the physique and distribution of fat and muscle tissue according to the female type are formed. The first menstruation (menarche) usually appears at the age of 12-13 years (±1.5-2 years). Cyclic processes and menstrual bleeding continue up to 45-50 years.
Since menstruation is the most pronounced external manifestation of the menstrual cycle, its duration is conventionally determined from the 1st day of the previous menstruation to the 1st day of the next menstruation.
Signs of the physiological menstrual cycle:
two-phase;
duration of no less than 21 and no more than 35 days (for 60% of women - 28 days);
cyclicity, and the cycle duration is constant;
duration of menstruation 2-7 days;
menstrual blood loss 50-150 ml;
6) absence of painful manifestations and disorders of the general condition of the body.
Regulation of the menstrual cycle
The reproductive system is organized according to a hierarchical principle. It has 5 levels, each of which is regulated by overlying structures using a feedback mechanism:
1) cerebral cortex;
2) subcortical centers located mainly in the hypothalamus;
3) brain appendage - pituitary gland;
4) gonads - ovaries;
5) peripheral organs (fallopian tubes, uterus and vagina, mammary glands).
Peripheral organs are the so-called target organs, since, due to the presence of special hormonal receptors in them, they most clearly respond to the action of sex hormones produced in the ovaries during the menstrual cycle. Hormones interact with cytosolic receptors, stimulating the synthesis of ribonucleoproteins (c-AMP), promoting the reproduction or inhibition of cell growth.
Cyclic functional changes occurring in a woman’s body are conditionally combined into several groups:
changes in the hypothalamus-pituitary system, ovaries (ovarian cycle);
the uterus and primarily in its mucous membrane (uterine cycle).
Along with this, cyclical shifts occur throughout the woman’s body, known as the menstrual wave. They are expressed in periodic changes in the activity of the central nervous system, metabolic processes, function of the cardiovascular system, thermoregulation, etc.
First level. Cortex.
In the cerebral cortex, the localization of the center that regulates the function of the reproductive system has not been established. However, through the cerebral cortex in humans, unlike animals, the external environment influences the underlying sections. Regulation is carried out through the amyhaloid nuclei (located in the thickness of the cerebral hemispheres) and the limbic system. In an experiment, electrical stimulation of the amyhaloid nucleus causes ovulation. In stressful situations with changes in climate and work rhythm, ovulation disturbance is observed.
Cerebral structures located in the cerebral cortex receive impulses from the external environment and transmit them using neurotransmitters to the neurosecretory nuclei of the hypothalamus. Neurotransmitters include dopamine, norepinephrine, serotonin, indole and a new class of morphine-like opioid neuropeptides - endorphins, enkephalins, donorphins. Function - regulate the gonadotropic function of the pituitary gland. Endorphins suppress the secretion of LH and reduce the synthesis of dopamine. Naloxone, an endorphin antagonist, leads to a sharp increase in the secretion of GT-RH. The effect of opioids is due to changes in dopamine levels.
Second level – pituitary zone of the hypothalamus
The hypothalamus is a part of the diencephalon and, through a number of nerve conductors (axons), is connected to various parts of the brain, due to which the central regulation of its activity is carried out. In addition, the hypothalamus contains receptors for all peripheral hormones, including ovarian hormones (estrogens and progesterone). Consequently, the hypothalamus is a kind of transfer point in which complex interactions take place between impulses entering the body from environment through the central nervous system, on the one hand, and the influence of hormones from the peripheral endocrine glands, on the other.
The hypothalamus contains nerve centers that regulate menstrual function in women. Under the control of the hypothalamus is the activity of the brain appendage - the pituitary gland, in the anterior lobe of which gonadotropic hormones are released that affect the function of the ovaries, as well as other tropic hormones that regulate the activity of a number of peripheral endocrine glands (adrenal cortex and thyroid gland).
The hypothalamic-pituitary system is united by anatomical and functional connections and is an integral complex that plays an important role in the regulation of the menstrual cycle.
The controlling effect of the hypothalamus on the anterior lobe of the adenohypophysis is carried out through the secretion of neurohormones, which are low molecular weight polypeptides.
Neurohormones that stimulate the release of tropic hormones of the pituitary gland are called releasing factors (from release - to release), or liberins. Along with this, there are also neurohormones that inhibit the release of tropic neurohormones - statins.
The secretion of RH-LH is genetically programmed and occurs in a certain pulsating mode with a frequency of 1 time per hour. This rhythm is called circharal (clockwise).
The circhoral rhythm was confirmed by direct measurement of LH in the portal system of the pituitary stalk and jugular vein in women with normal function. These studies made it possible to substantiate the hypothesis about the triggering role of RH-LH in the function of the reproductive system.
The hypothalamus produces seven releasing factors, leading to the release of the corresponding tropic hormones in the anterior pituitary gland:
somatotropic releasing factor (SRF), or somatoliberin;
adrenocorticotropic releasing factor (ACTH-RF), or corticoliberin;
thyroid-stimulating releasing factor (TRF), or thyrotropin-releasing hormone;
melanoliberin;
follicle-stimulating releasing factor (FSH-RF), or folliberin;
luteinizing releasing factor (LRF), or luliberin;
prolactin-releasing factor (PRF), or prolactoliberin.
Of the listed releasing factors, the last three (FSG-RF, L-RF and P-RF) have direct relation to the implementation of menstrual function. With their help, three corresponding hormones - gonadotropins - are released in the adenohypophysis, since they have an effect on the gonads - the sex glands.
To date, only two factors have been discovered that inhibit the release of tropic hormones and statins in the adenohypophysis:
somatotropin-inhibiting factor (SIF), or somatostatin;
prolactininhibiting factor (PIF), or prolactostatin, which is directly related to the regulation of menstrual function.
Hypothalamic neurohormones (liberins and statins) enter the pituitary gland through its stalk and portal vessels. A feature of this system is the possibility of blood flow in both directions, due to which a feedback mechanism is implemented.
The circhoral mode of RH-LH release is formed at puberty and is an indicator of the maturity of the neurostructures of the hypothalamus. Estradiol plays a certain role in regulating the release of RH-LH. In the preovulatory period, against the background of the maximum level of estradiol in the blood, the magnitude of the release of RG-LH is significantly higher in the early foliculin and luteal phase. It has been proven that thyroliberin stimulates the release of prolactin. Dopamine inhibits the release of prolactin.
Third level – anterior pituitary gland (FSH LH, prolactin)
The pituitary gland is the most structurally and functionally complex endocrine gland, consisting of the adenohypophysis (anterior lobe) and the neurohypophysis (posterior lobe).
The adenohypophysis secretes gonadotropic hormones that regulate the function of the ovaries and mammary glands: lutropin (luteinizing hormone, LH), follitropin (follicle-stimulating hormone, FSH), prolactin (PrL) and also somatotropin (STH), corticotropin (ACTH), thyrotropin (TSH).
In the pituitary cycle, two functional phases are distinguished - follicular, with predominant secretion of FSH, and luteal, with dominant secretion of LH and PrL.
FSH stimulates follicle growth and proliferation of granulosa cells in the ovary; together with LH, it stimulates the release of estrogens and increases the content of aromatase.
An increase in LH secretion with a mature dominant follicle causes ovulation. LH then stimulates the corpus luteum to release progesterone. The dawn of the corpus luteum is determined by the additional influence of prolactin.
Prolactin, together with LH, stimulates the synthesis of progesterone by the corpus luteum; its main biological role is the growth and development of the mammary glands and the regulation of lactation. In addition, it has a fat-mobilizing effect and lowers blood pressure. An increase in prolactin in the body leads to disruption of the menstrual cycle.
Currently, two types of gonadotropin secretion have been discovered: tonic, promoting the development of follicles and their production of estrogens, and cyclical, ensuring a change in phases of low and high concentrations of hormones and, in particular, their preovulatory peak.
Level four - ovaries
The ovary is an autonomous endocrine gland, a kind of biological clock in a woman’s body that implements a feedback mechanism.
The ovary performs two main functions - generative (maturation of follicles and ovulation) and endocrine (synthesis of steroid hormones - estrogens, progesterone and, in a small amount, androgens).
The process of folliculogenesis occurs continuously in the ovary, starting in the antenatal period and ending in postmenopause. In this case, up to 90% of the follicles become atretic and only a small part of them goes through the full development cycle from primordial to mature and turns into the corpus luteum.
At the birth of a girl, both ovaries contain up to 500 million primordial follicles. By the beginning of adolescence, due to atresia, their number is halved. During the entire reproductive period of a woman's life, only about 400 follicles mature.
The ovarian cycle consists of two phases - follicular and luteal. The follicular phase begins after the end of menstruation and ends with ovulation; luteal - begins after ovulation and ends with the appearance of menstruation.
Typically, from the beginning of the menstrual cycle to the 7th day, several follicles begin to grow simultaneously in the ovaries. From the 7th day, one of them is ahead of the others in development, by the time of ovulation it reaches a diameter of 20-28 mm, has a more pronounced capillary network and is called dominant. The reasons why the selection and development of a dominant follicle occurs have not yet been clarified, but from the moment of its appearance, other follicles stop their growth and development. The dominant follicle contains an egg, its cavity is filled with follicular fluid.
By the time of ovulation, the volume of follicular fluid increases 100 times, the content of estradiol (E 2) sharply increases in it, the rise in the level of which stimulates the release of LH by the pituitary gland and ovulation. The follicle develops in the first phase of the menstrual cycle, which lasts on average until the 14th day, and then the mature follicle ruptures - ovulation.
Shortly before ovulation, the first meiosis occurs, i.e., reduction division of the egg. After ovulation, the egg from the abdominal cavity enters the fallopian tube, in the ampullary part of which the second reduction division occurs (second meiosis). After ovulation, under the influence of the predominant effect of LH, further proliferation of granulosa cells and connective tissue membranes of the follicle and accumulation of lipids in them are observed, which leads to the formation of the corpus luteum 1.
The process of ovulation itself is a rupture of the basement membrane of the dominant follicle with the release of the egg, surrounded by the corona radiata, into the abdominal cavity and subsequently into the ampullary end of the fallopian tube. If the integrity of the follicle is damaged, slight bleeding occurs from the destroyed capillaries. Ovulation occurs as a result of complex neurohumoral changes in a woman’s body (the pressure inside the follicle increases, its wall becomes thinner under the influence of collagenase, proteolytic enzymes, prostaglandins).
The latter, as well as oxytocin and relaxin, change the vascular filling of the ovary and cause contraction of the muscle cells of the follicle wall. The ovulation process is also influenced by certain immune changes in the body.
An unfertilized egg dies after 12-24 hours. After its release into the cavity of the follicle, the forming capillaries quickly grow, granulosa cells undergo luteinization - a corpus luteum is formed, the cells of which secrete progesterone.
In the absence of pregnancy, the corpus luteum is called menstrual; its blossoming stage lasts 10-12 days, and then reverse development and regression occurs.
The inner membrane, granulosa cells of the follicle, and the corpus luteum, under the influence of pituitary hormones, produce sex steroid hormones - estrogens, gestagens, androgens, the metabolism of which is carried out mainly in the liver.
Estrogens include three classical fractions - estrone, estradiol, estriol. Estradiol (E 2) is the most active. In the ovary and early follicular phase, 60-100 mcg is synthesized, in the luteal phase - 270 mcg, by the time of ovulation - 400-900 mcg / day.
Estrone (E 1) is 25 times weaker than estradiol, its level from the beginning of the menstrual cycle to the moment of ovulation increases from 60-100 mcg/day to 600 mcg/day.
Estriol (Ez) is 200 times weaker than estradiol and is a low-active metabolite of Ei and E2.
Estrogens (from oestrus - estrus), when administered to castrated female white mice, cause them to estrus - a condition similar to that occurring in uncastrated females during spontaneous maturation of the egg.
Estrogens promote the development of secondary sexual characteristics, regeneration and growth of the endometrium in the uterus, preparation of the endometrium for the action of progesterone, stimulate the secretion of cervical mucus, and the contractile activity of the smooth muscles of the genital tract; change all types of metabolism with a predominance of catabolic processes; lower body temperature. Estrogens in physiological quantities stimulate the reticuloendothelial system, enhancing the production of antibodies and the activity of phagocytes, increasing the body's resistance to infections; retain nitrogen, sodium, liquid in soft tissues, and calcium and phosphorus in bones; cause an increase in the concentration of glycogen, glucose, phosphorus, creatinine, iron and copper in the blood and muscles; reduce the content of cholesterol, phospholipids and total fat in the liver and blood, accelerate the synthesis of higher fatty acids. Under the influence of estrogens, metabolism occurs with a predominance of catabolism (retention of sodium and water in the body, increased dissimilation of proteins), and a decrease in body temperature, including basal temperature (measured in the rectum), is also observed.
The process of development of the corpus luteum is usually divided into four phases: proliferation, vascularization, flowering and reverse development. By the time the corpus luteum reverses its development, the next menstruation begins. If pregnancy occurs, the corpus luteum continues to develop (up to 16 weeks).
Gestagens (from gesto - to wear, to be pregnant) contribute to the normal development of pregnancy. Progestins, produced mainly by the corpus luteum of the ovary, play a large role in the cyclic changes in the endometrium that occur in the process of preparing the uterus for implantation of a fertilized egg. Under the influence of gestagens, the excitability and contractility of the myometrium are suppressed while simultaneously increasing its extensibility and plasticity. Progestogens, together with estrogens, play an important role during pregnancy in preparing the mammary glands for the upcoming lactation function after childbirth. Under the influence of estrogens, proliferation of the mammary ducts occurs, and gestagens act mainly on the alveolar apparatus of the mammary glands.
Gestagens, in contrast to estrogens, have an anabolic effect, that is, they promote the absorption (assimilation) by the body of substances, in particular proteins, coming from outside. Gestagens cause a slight increase in body temperature, especially basal.
Progesterone is synthesized in the ovary in an amount of 2 mg/day in the follicular phase and 25 mg/day. - into the luteal. Progesterone is the main gestagen of the ovaries; the ovaries also synthesize 17a-hydroxyprogesterone, D 4 -pregnenol-20-OH-3, O 4 -pregnenol-20-OH-3.
Under physiological conditions, gestagens reduce the content of amine nitrogen in the blood plasma, increase the secretion of amino acids, increase the secretion of gastric juice, and inhibit bile secretion.
The following androgens are produced in the ovary: androstenedione (a precursor of testosterone) in an amount of 15 mg/day, dehydroepiandrosterone and dehydroepiandrosterone sulfate (also precursors of testosterone) in very small quantities. Small doses of androgens stimulate the function of the pituitary gland, large doses block it. The specific effect of androgens can manifest itself in the form of a virile effect (hypertrophy of the clitoris, male hair growth, proliferation of the cricoid cartilage, the appearance of acne vulgaris), an antiestrogenic effect (in small doses they cause proliferation of the endometrium and vaginal epithelium), a gonadotropic effect (in small doses they stimulate the secretion of gonadotropins , promote growth, maturation of the follicle, ovulation, formation of the corpus luteum); antigonadotropic effect (high concentration of androgens in the preovulatory period suppresses ovulation and subsequently causes follicular atresia).
The granulosa cells of the follicles also produce the protein hormone inhibin, which inhibits the release of FSH by the pituitary gland, and local protein substances - oxytocin and relaxin. Oxytocin in the ovary promotes regression of the corpus luteum. The ovaries also produce prostaglandins. The role of prostaglandins in the regulation of the female reproductive system is to participate in the process of ovulation (they ensure rupture of the follicle wall by increasing the contractile activity of the smooth muscle fibers of the follicle shell and reducing the formation of collagen), in the transport of the egg (they influence the contractile activity of the fallopian tubes and affect the myometrium, promoting nidation blastocysts), in the regulation of menstrual bleeding (the structure of the endometrium at the time of its rejection, the contractile activity of the myometrium, arterioles, platelet aggregation are closely related to the processes of synthesis and breakdown of prostaglandins).
Prostaglandins are involved in the regression of the corpus luteum, if fertilization does not occur.
All steroid hormones are formed from cholesterol; gonadotropic hormones participate in the synthesis: FSH and LH and aromatase, under the influence of which estrogens are formed from androgens.
All of the above cyclic changes occurring in the hypothalamus, the anterior lobe of the pituitary gland and the ovaries are now commonly referred to as the ovarian cycle. During this cycle, complex relationships occur between the hormones of the anterior pituitary gland and peripheral sex (ovarian) hormones. These relationships are shown schematically in Fig. 1, from which it is clear that the greatest changes in the secretion of gonadotropic and ovarian hormones occur during the maturation of the follicle, the onset of ovulation and the formation of the corpus luteum. Thus, by the time of ovulation, the greatest production of gonadotropic hormones (FSH and LH) is observed. The production of estrogen is associated with the maturation of the follicle, ovulation and partly with the formation of the corpus luteum. The formation and increase in activity of the corpus luteum is directly related to the production of gestagens.
Under the influence of these ovarian steroid hormones, basal temperature changes; with a normal menstrual cycle, its distinct two-phase nature is noted. During the first phase (before ovulation), the temperature is several tenths of a degree below 37°C. During the second phase of the cycle (after ovulation), the temperature rises a few tenths of a degree above 37°C. Before the start of the next menstruation and during its process, the basal temperature again drops below 37°C.
The hypothalamus - pituitary gland - ovaries system is a universal, self-regulating supersystem that exists through the implementation of the feedback law.
The law of feedback is the basic law of the functioning of the endocrine system. There are negative and positive mechanisms. Almost always during the menstrual cycle a negative mechanism operates, according to which a small amount of hormones in the periphery (ovary) causes the release of high doses of gonadotropic hormones , and with an increase in the concentration of the latter in the peripheral blood, stimuli from the hypothalamus and pituitary gland decrease.
The positive mechanism of the feedback law is aimed at providing an ovulatory LH peak, which causes rupture of the mature follicle. This peak is due to the high concentration of estradiol produced by the dominant follicle. When the follicle is ready to rupture (similar to how the pressure in a steam boiler increases), the “valve” in the pituitary gland opens and a large amount of LH is simultaneously released into the blood.
The feedback law is carried out along a long loop (ovary - pituitary gland), short (pituitary gland - hypothalamus) and ultra-short (gonadotropin-releasing factor - neurocytes of the hypothalamus).
In the regulation of menstrual function, the implementation of the principle of so-called feedback between the hypothalamus, the anterior pituitary gland and the ovaries is of great importance. It is customary to consider two types of feedback: negative and positive. At negative type of feedback the production of central neurohormones (releasing factors) and gonadotropins of the adenohypophysis is suppressed by ovarian hormones produced in large quantities. At positive type of feedback The production of releasing factors in the hypothalamus and gonadotropins in the pituitary gland is stimulated by low levels of ovarian hormones in the blood. The implementation of the principle of negative and positive feedback underlies the self-regulation of the function of the hypothalamus-pituitary-ovarian system.
Cyclic processes under the influence of sex hormones also occur in other target organs, which in addition to the uterus include the tubes, vagina, external genitalia, mammary glands, hair follicles, skin, bones, and adipose tissue. The cells of these organs and tissues contain receptors for sex hormones.
These receptors are found in all structures of the reproductive system, in particular in the ovaries - in the granulosa cells of the maturing follicle. They determine the sensitivity of the ovaries to pituitary gonadotropins.
Breast tissue contains receptors for estradiol, progesterone, prolactin, which ultimately regulate milk secretion.
Fifth level – target tissues
Target tissues are the points of application of the action of sex hormones: genital organs: uterus, tubes, cervix, vagina, mammary glands, hair follicles, skin, bones, adipose tissue. The cytoplasm of these cells contains strictly specific receptors for sex hormones: estradiol, progesterone, testosterone. These receptors are found in the nervous system.
Of all the target organs, the greatest changes occur in the uterus.
In connection with the process of reproduction, the uterus consistently performs three main functions: menstrual, necessary to prepare the organ and especially the mucous membrane for pregnancy; the function of the fruit receptacle to ensure optimal conditions for the development of the fetus and the fetal expulsion function during childbirth.
Changes in the structure and function of the uterus as a whole, and especially in the structure and function of the endometrium, which occur under the influence of ovarian sex hormones, are called uterine cycle. During the uterine cycle, there is a sequential change of four phases of cyclic changes in the endometrium:
1) proliferation; 2) secretion; 3) desquamation (menstruation); 4) regeneration. The first two phases are considered as the main ones. That is why the normal menstrual cycle is usually called two-phase. The known boundary between these two main phases of the cycle is ovulation. There is a clear relationship between the changes occurring in the ovary before and after ovulation, on the one hand, and the consistent change of phases in the endometrium, on the other (Fig. 4).
First main proliferation phase endometrium begins after the completion of regeneration of the mucous membrane that was rejected during the previous menstruation. The functional (superficial) layer of the endometrium, which arises from the remains of the glands and stroma of the basal part of the mucous membrane, participates in regeneration. The beginning of this phase is directly related to the increasing effect on the uterine mucosa of estrogens produced by the maturing follicle. At the beginning of the proliferation phase, the endometrial glands are narrow and smooth (Fig. 5, a). As proliferation increases, the glands increase in size and begin to flex slightly. The most pronounced proliferation of the endometrium occurs at the time of complete maturation of the follicle and ovulation (days 12-14 of the 28-day cycle). The thickness of the uterine mucosa by this time reaches 3-4 mm. This ends the proliferation phase.

Rice. 4. The relationship between changes in the ovaries and the uterine lining during the normal menstrual cycle.
1 - maturation of the follicle in the ovary - proliferation phase in the endometrium; 2 - ovulation; 3 - formation and development of the corpus luteum in the ovary - secretion phase in the endometrium; 4 - reverse development of the corpus luteum in the ovary, rejection of the endometrium - menstruation; 5 - the beginning of the maturation of a new follicle in the ovary - the regeneration phase in the endometrium.
Second main secretion phase endometrial glands begins under the influence of the rapidly increasing activity of gestagens produced in increasing quantities by the corpus luteum of the ovary. The endometrial glands wriggle more and more and are filled with secretions (Fig. 5, b). The stroma of the uterine mucosa swells and is pierced by spirally convoluted arterioles. At the end of the secretion phase, the lumens of the endometrial glands acquire a sawtooth shape with the accumulation of secretion, glycogen content and the appearance of pseudodecidual cells. It is by this time that the uterine mucosa is fully prepared to receive a fertilized egg.
If, after ovulation, fertilization of the egg does not occur and, accordingly, pregnancy does not occur, the corpus luteum begins to undergo reverse development, which leads to a sharp decrease in the content of estrogen and progesterone in the blood. As a result, foci of necrosis and hemorrhage appear in the endometrium. Then the functional layer of the uterine mucosa is shed and the next menstruation begins, which is the third phase of the menstrual cycle - desquamation phase, lasting on average about 3-4 days. By the time menstrual bleeding stops, the fourth (final) phase of the cycle begins - regeneration phase, lasting 2-3 days.
The phase changes described above in the structure and function of the mucous membrane of the uterine body are reliable manifestations of the uterine cycle.

