Testing the physical performance of persons involved in physical education and sports at rest does not reflect its functional state and reserve capabilities, since the pathology of an organ or its functional failure manifests itself more noticeably under load conditions than at rest, when the requirements for it are minimal. Unfortunately, the function of the heart, playing a leading role in the life of the body, in most cases is assessed on the basis of an examination at rest. Although it is obvious that any violation of the pumping function of the heart is more likely to manifest itself at a minute volume of 12-15 l/min than at 5-6 l/min. In addition, insufficient reserve capabilities of the heart can only manifest themselves in work that exceeds the usual load in intensity. This also applies to latent coronary insufficiency, which is often not diagnosed by ECG at rest. Therefore, assessment of the functional state of the cardiovascular system at the modern level is impossible without the widespread use of stress tests. Load test objectives: 1) determination of performance and suitability for practicing a particular sport; 2) assessment of the functional state of the cardiorespiratory system and its reserves; 3) forecasting of likely sports results, as well as forecasting the likelihood of certain deviations in health status when undergoing physical activity; 4 ) determination and development of effective preventive and rehabilitation measures for highly qualified athletes; 5) assessment of the functional state and effectiveness of the use of rehabilitation means after injuries and diseases in training athletes. Recovery tests.Recovery tests involve taking into account changes and determining the recovery time after standard physical activity in such indicators of the cardiorespiratory system as heart rate (HR), blood pressure (BP), electrocardiogram (EKG) readings, respiratory rate (RR) and many others.B sports medicine uses V.V. samples. Gorinevskgo (60 jumps for 30 s), Deshin and Kotov test (three-minute running in place at a pace of 180 steps per minute), Martinet test (20 squats) and other functional tests. When conducting each of these tests, heart rate and blood pressure are taken into account before the load and after its completion at the 1st, 2nd, 3rd and 4th minutes. Recovery tests also include various versions of the step-test In 1925, A. Master introduced a two-stage test, where heart rate and blood pressure were also recorded after a certain number of climbs to a standard step. Later, this test began to be used to record ECG after exercise (A. Master and H. Jafte, 1941). In its modern form, a two-stage test provides for a certain number of rises on a standard double step for 1.5 minutes, depending on the age, gender and body weight of the subject (see table. Minimum number of rises per step), or double the number of rises in 3 minutes with a double sample (the height of each step is 23 cm). ECG is recorded before and after exercise Submaximal effort tests.Submaximal force tests are used in sports medicine when testing highly skilled athletes. Studies have shown that the most valuable information about the functional state of the cardiorespiratory system can be obtained by taking into account changes in the main hemodynamic parameters (indicators) not in the recovery period, but directly during the test. Therefore, an increase in loads is carried out until the limit of aerobic capacity is reached (maximum oxygen consumption - MOC). In sports medicine, submaximal load tests are also used, requiring 75% of the maximum tolerated load. They are recommended by WHO for widespread use (WHO Chronicle, 1971, 25/8, p. 380, etc.). Various bicycle ergometers, treadmills, etc. are also used (Fig. Examination on a treadmill). If the age limits of the heart rate are exceeded (see table. Maximum permissible heart rate during the stress test), it is advisable to stop the load. Submaximal stress tests.Submaximal exercise tests are carried out with different types of loads: 1) immediately increasing the load after warming up to the expected submaximal level for a given subject; 2) uniform load at a certain level with an increase in subsequent studies; 3) continuous or almost continuous increase in load; 4) stepwise increase in load;
5) stepwise increase in load, alternating with periods of rest. The first, third and fourth tests are used mainly when examining athletes, the second - for a comparative assessment of the tolerance of a certain load by any group of individuals. According to WHO recommendations, when examining healthy individuals, the initial load in women should be 150 kgm/min, followed by an increase to 300-450-600 kgm/min, etc.; for men - 300 kgm/min, followed by an increase to 600-900-1200 kgm/min, etc. The duration of each load stage is at least 4 minutes. Rest periods between load stages are 3-5 minutes. The treadmill test (see Fig. Treadmill Test) usually starts at a speed of 6 km/h and then increases to 8 km/h, 10 km/h, etc. The movement slope increases stepwise to 2.5%. Bicycle ergometry.The bicycle ergometer is the most convenient device for conducting submaximal load tests, as it provides the optimal opportunity to obtain accurate physiological data to assess the functional state of a person and his physical abilities. The pedaling speed is usually 60 rpm. During the examination, constant monitoring of heart rate, blood pressure, and ECG is necessary.
Question 28. It is necessary to clearly distinguish between acute and chronic “heart strain.” These are different conditions. Acute cardiac overstrain can manifest itself in different ways - sometimes as acute heart failure, which occurs during or immediately after physical activity that is excessive for a given person, especially if it is performed in a painful state (flu, sore throat), or in case of violation of the regime (drinking alcohol, smoking), after “weight loss,” etc. Mention should also be made of acute heart failure, which occurs during exercise due to the acute development of pulmonary emphysema. The clinical picture of acute heart failure, as well as acute vascular failure (gravitational shock, collapse, etc.), in athletes, in fact, does not differ from such conditions in those not involved in sports and is described in detail in the relevant literature, as well as medical tactics for these conditions [Weisbein S.G., 1957; Dobrovolsky V.K., I960, etc.]. With acute physical overstrain, coronary circulation disorders may occur (for example, a paradoxical reaction of coronary vessels reacting with spasm instead of dilatation, myocardial infarction, hemorrhage into the heart muscle, etc.). In addition, acute cardiac overstrain can also manifest as myocardial dystrophy, sometimes to such an extent that is incompatible with life. A classic example of such an outcome is the death of the Greek warrior Feidipius, described more than 3000 years ago, who ran 42 km 195 m to Athens to report the good news of the victory at Marathon. Thus, myocardial dystrophy is one of the possible manifestations of acute cardiac overstrain. Acute myocardial dystrophy can occur in isolation in both the left and right ventricles. In the clinic, acute overstrain of the left ventricle is often observed with a sudden increase in blood pressure in the systemic circulation (acute nephritis, hypertensive crisis), that is, in cases where the left ventricle is forced to overcome this acutely increased resistance. Acute right ventricular strain occurs when there is a sudden increase in vascular resistance in the pulmonary artery, for example during pulmonary embolism. Various options for the heart's response to acute physical stress are usually accompanied by a corresponding clinical picture (angina pectoris, myocardial infarction, cardiac asthma, etc.). However, acute myocardial dystrophy may not give a picture of heart failure and manifest itself only by ECG changes. We are talking either only about a decrease in the height of the T wave, mainly in the chest leads, or about changes in the final part of the ventricular complex with its initial part unchanged, consisting in a displacement of the ST segment downward with a convexity upward and in the inversion of unequal T waves in various leads (depending on localization of these changes in the myocardium). Such acute changes were called “heart-strain” in the Anglo-American literature, i.e. “heart strain.” Before they were identified as an independent syndrome, such ECG changes were regarded (and are often regarded now) as hypertrophy of certain parts of the heart or as coronary insufficiency. The identification of ECG cardiac overstrain syndrome, which occurs acutely in patients, forced a new look some ECG changes that sometimes occur in athletes and are fully consistent with the described ECG picture of the patients. It should be noted that in athletes any pathological changes in the myocardium are unlikely. Thus, there is no doubt that changes in the heart during physical overstrain occur in healthy myocardium. A thorough clinical analysis of this kind of ECG changes in athletes [Dembo A. G. et al., 1960-1988] showed that only a few these acutely occurring changes are of coronary origin. In most cases, they are a manifestation of myocardial dystrophy due to excessive load that does not correspond to the body’s capabilities.
Question 29. Physiological features of sports training for women physiological reactions to physical activity, as well as the mechanisms that determine the functional capabilities of the body and their changes under the influence of sports training, are not fundamentally different in women and men. Some quantitative differences between them are well illustrated by the ratio of world sports records. Record results for women at running distances are 8-13% lower than for men. In swimming, women's records are somewhat closer to men's than in running (the difference is 6-10 %). Dependence of the functional capabilities of the body on body size. When When comparing functional indicators in women and men, differences in body size should first be taken into account. On average, women are shorter than men. Even just because of these differences, under all other identical conditions, many functional indicators in women, in particular their performance, should differ from the corresponding indicators in men. (The same is true when comparing children and adults of different body sizes.) P Let's compare functional capabilities of a woman 160 cm tall and a man 176 cm tall, assuming that all their linear dimensions are proportional to body length (b). A man is 1.1 times taller than a woman (176: 160). In this case, all linear dimensions, i.e. the length of all parts of the body and limbs, the length of levers (distances from the axis of rotation of the joint to the place of muscle attachment), amplitude of movements, etc., in a man are 1.1 times greater than in a woman. The surface dimensions are proportional to the square of the linear dimensions (L2). Therefore, the cross-sectional area of the muscles, aorta, body surface, and alveolar surface of the lungs in this example in a man should be 1.21 times larger (1.12) than in a woman. Volumetric dimensions are proportional to the cube of linear dimensions (L3). Therefore, the lung volume, circulating blood volume or heart volume of a man should be 1.33 times greater (1.13) than that of a woman. Body mass (weight) (M) is also proportional to L3, so under other different conditions, the weight of a man should be 1.33 times greater than the weight of a woman. The maximum force (F) that muscles are capable of developing is proportional to their cross-sectional area, i.e. L2 In this example, the maximum force of muscle contraction in men should be 1.21. times more than in women. a man is able to do a lot of work - in this example, 1.33 times. T Thus, the difference in body size should itself in itself predetermine gender differences in performance, which are not associated with any special functional differences in the body of women and men. The work performed at a certain power must be ensured by an equivalent supply of chemical energy (oxygen) to the working muscles. Therefore, energy expenditure (rate of O2 consumption) should be related to the mass of working muscles and body weight. From theoretical premises it should be expected that the maximum O2 consumption should be proportional to L2 or M2/3. It is differences in body size (body weight and muscle mass) that primarily explain the higher BMD values in men compared to women. Usually, to compare MIC in different people, a relative indicator is used - MIC divided by body weight (ml/kg * min). However, it is more correct (more accurate) to compare MIC in people with different body weights, expressing MIC in ml / kg / z * in. Cardiac output (Q) is determined by the volume of blood pumped by the heart per unit time. Accordingly, the maximum cardiac output should be proportional to L2 or M2/3 Pulmonary ventilation (Vе), as the product of tidal volume and respiratory rate, is proportional to the square of the linear dimensions of the body (L2). Lung volumes in women and men of different ages correspond to body sizes (proportional to L3). Differences in lung size are determined mainly (if not exclusively) by sex differences in linear body size. There are significant differences in body composition between women and men. In adult men, muscle mass makes up about 40% of body weight (average about 30 kg), and in women it is about 30% (average 18 kg). Thus, in both absolute and relative terms, muscle mass in women is significantly less than in men. The total amount of adipose tissue in women averages about 25%, and in men - about 15% of body weight. The absolute amount of fat in women is also greater than in men, by about 4-8 kg. Lean body mass (body weight minus weight adipose tissue), which consists mainly of muscles, as well as bones and internal organs, is 15-20 kg less in women than in men. Athletes have lower fat content than untrained women, but even very good athletes - long-distance runners - can only reach the level typical of untrained men. In most sports, the bulk of physical activity involves moving your own body weight. Therefore, excess adipose tissue in the body constitutes an additional load, for example, in running or jumping, but not in swimming. Since adipose tissue contains almost no water, the total body water content in women is significantly less than in men (about 55 and 70%, respectively). body weight).
Question 30. Physiological classification of physical exercises Group I - standard. Cyclic: maximum power; submaximal; large; moderate. Acyclic: one-time; combinations. Group II - non-standard. The group of standard exercises is performed under relatively constant conditions. Under these conditions, the athlete strives to either practice or maintain the constancy of previously acquired motor skills. This group of exercises includes movements used in running, swimming, gymnastics, weightlifting, etc. For example, during track and field running, the performer has a specific motor task that he knows: to run 100 m. The set of movements performed in this case has already been previously worked out .You need to perform these movements within a given period of time. Another group of physical exercises is performed under non-standard conditions, with constantly changing tasks. Movements here depend on an unforeseen change in the situation created at the moment. For example, the motor act of a fencer depends on the nature of the movement of his opponent. When performing non-standard physical exercises the load on the central nervous system will be significantly greater than in the first group (standard movements). The speaker is required to quickly solve continuously changing motor tasks. To perform them, greater mobility of nervous processes is required. In adolescence, as is known, endocrine changes occur, which in some cases creates instability in nervous processes. In this regard, during medical supervision, special attention should be paid to adolescents performing non-standard physical exercises of high intensity. To the group of non-standard exercises These include movements found in martial arts (boxing, wrestling, fencing), as well as in sports games (volleyball, football, basketball, hockey, etc.). These sports primarily develop agility.
Question 32. Posture(lat. positum put, pose; fr: pose) - the position taken by the human body, the position of the body, head and limbs in relation to each other. Contents [remove] In a figurative meaning - pretense, insincere behavior, panache (for example, “Become into a pose" - take a deliberately spectacular position). The pose is characterized by relative immobility. Common human postures are orthograde (standing, sitting) and horizontal (lying, on all fours). Studied in biomechanics, physical education and physiology. Posture is usually maintained through the balance of body segments, tonic tension of the muscles supporting the articular angles, and interaction with the support. Regulation of posture is complex and is carried out with the participation of various levels of the central nervous system, and with voluntary changes in posture, the cerebral cortex. The sense of posture is proprioception. In both humans and animals, posture can express emotions. Emotions are also conveyed through posture in art - ballet, sculpture, painting. Particular importance is attached to posture in sports (including martial arts), in health systems (for example, in yoga) and in medicine. The term “posture” is associated with a number of rather complex concepts from the field of physical culture, physiology and human biomechanics: posture body, posture, standing, walking. General characteristics of the pose. Natural pose- a relaxed, ordinary pose, taken without any effort on the part of the person taking it. Unnatural pose- a pose that is not typical for a living healthy person in consciousness (the pose of a corpse, a characteristic pose (opisthotonus) for tetanus, unnatural pretentious poses for schizophrenia). Unnatural postures associated with diseases are classified as pathological postures. Pathological posture- posture as a result of a disease of the musculoskeletal or nervous system. Forced pose- a posture taken under the influence of external circumstances or to relieve pain (for example, a forced working posture, antalgic posture for lumbar radiculitis) Habitual pose- a feature of the posture of a particular person, which he takes without excessive muscle tension, automatically, without the participation of consciousness (see posture). There are also such separate concepts as “working posture”, “sports posture”...
Question 35. Classification of acyclic exercises. A cyclic competitive exercises based on their kinematic and dynamic characteristics can be divided into 1) explosive, 2) standard-variable, 3) non-standard-variable and 4) interval-repetitive). Explosive exercises. Explosive exercises include jumping and throwing. The group of jumps includes jumps in athletics (long, high, triple, pole), ski jumping and ski jumping in water skiing, diving, gymnastic and acrobatic jumps. The Throwing group includes athletics throwing: discus, javelin, hammer, shot put. A special case of throwing is weightlifting exercises (snatch and clean and jerk). X characteristic feature of explosive exercises - the presence of one or more accentuated short-term efforts of high power (“explosion”), imparting high speed to the entire body and (or) upper limbs with a sports equipment. These explosive muscle efforts determine: a) the distance of the long or high jump; b) the duration of the flight, during which complex movements are performed in the air (diving, gymnastic and acrobatic jumps); c) the maximum (in track and field throwing) or required (in weightlifting exercises) flight range of a sports projectile. All explosive exercises have a very short duration - from a few seconds to a few tens of seconds. A significant part of most explosive exercises are cyclic movements - run-up or acceleration. Each explosive exercise is performed as a single whole, which determines the features of teaching such movements. WITH standard variable exercises- these are competitive exercises in sports and rhythmic gymnastics and acrobatics (except jumping), in figure skating and water skiing, in synchronized swimming. These exercises are characterized by the combination into a continuous, strictly fixed, standard chain of various complex actions (elements), each of which is a complete independent action and therefore can be learned separately and included as a component in a variety of combinations (complex exercises). N estandard-variables(situational) exercises include all sports games and combat sports, as well as all types of alpine skiing. During the execution of these exercises, periods with different character and intensity of motor activity alternate sharply and in a non-standard way - from short-term maximum efforts of an explosive nature (accelerations, jumps, strikes) to physical activity of relatively low intensity, up to complete rest (minute breaks for boxers and wrestlers , stoppages in play, rest periods between halves in sports games). In this regard, in non-standard-variable exercises one can distinguish working periods, i.e. periods of particularly intense motor activity (activity), and intermediate periods, or periods of relatively low-intensity motor activity. TO interval-repetition exercises include competitive as well as complex training exercises, which are composed of a standard combination of different or identical elements, separated by periods of complete or partial rest. Moreover, the elements included in such a combination can be homogeneous (in nature and intensity) cyclic or acyclic exercises. Thus, interval-repetitive exercises include a training exercise with repeated running (swimming) of certain sections of a distance at high speed, alternating with periods of complete or partial rest. Another example is lifting a barbell several times in a row. Competitive interval-repetition exercises include biathlon and orienteering. If, during complex training exercises, work periods alternate with intermediate periods of complete rest, then such exercises are designated as repeated variable exercises*.
Question 36. Recreational swimming A person immersed in water loses as much weight as the liquid he displaced weighs. Practical weighing showed: a person of average size weighs 2-3 kg in water. This is the basis of one of the healing properties of swimming. "Hydraulic weightlessness » allows you to relieve the spine, the intervertebral discs straighten and rest. Exceptionally favorable conditions arise for enhancing metabolism. A person grows, as they say, before our eyes. Measure your height before diving into the pool, and after 45 minutes of swimming, you will gain an extra centimeter, or even more. Children who swim a lot and regularly grow faster. Swimming is recommended as a remedy for various curvatures of the spine and postural defects. With any method of swimming, almost all joints of the spine act with high amplitude and in a variety of planes, making full use of their natural capabilities. At the same time, the limits of possibilities are somewhat expanded, and the joints of the spine no longer bear a heavy static support load. A person immersed in water spends almost no effort maintaining his position. A swimmer works lying down. Correct swimming technique allows you to evenly load the muscles of the spine. With different methods of swimming, the work of the spine has its own specifics. In all methods of swimming, it is necessary to master a deep and quick breath. This requires excellent chest mobility. Spirometry readings in swimmers are much higher than those of non-swimmers of the same height and weight. This is an extremely important point. It has been established that with age, the vital capacity of a person’s lungs steadily decreases. Why? When answering this question, they usually forget about the main reason - a decrease in the range of motion of the rib joints and the thoracic spinal column. In older people, the mobility of the difficult cell is only 1-2 cm or even completely disappears. Gradually, the so-called abdominal type of breathing is formed, in which inhalation occurs solely due to the lowering of the dome of the diaphragm. Swimming allows you to use the rib joints and spine for their intended purpose until old age and maintain youthful mobility of the lungs (10-16 cm), excellent flexibility of the spine, preventing the development of osteochondrosis. Before swimming training, do warm-up exercises. Swimmers call it “dry swimming” and perform it after warming up and before entering the water. In your set of dry swimming gymnastic exercises, be sure to include more strength exercises that do not require a large range of motion. Thanks to them, the muscles, having received additional opportunities for stretching, retain a sufficiently high tone and the ability to withstand traumatic force in emergency cases. Having learned to float on the water, begin to study sports swimming styles, which are extremely useful, including in terms of health benefits. Remember to breathe correctly and exercise the chest joints during forced inhalation and exhalation. Don’t forget about general physical training, especially strength exercises of moderate amplitude. When you decide to take up swimming, remember that even swimming poorly is better than not swimming at all.
Question 37. Dynamics of the physiological state of the body during sports activity. When performing a training or competitive exercise, significant changes occur in the athlete’s functional state. In the continuous dynamics of these changes, three main periods can be distinguished: pre-start, main (working) and recovery (Fig. 9). The pre-start state is characterized by functional changes preceding the start of work (exercise). In the working period, a distinction is made between rapid changes in functions in the very initial period of work - the working state and the following relatively unchanged (or rather, slowly changing) state of the basic physiological functions, the so-called steady state. In the process of performing the exercise, fatigue develops, which manifests itself in a decrease in performance, i.e., the inability to continue the exercise at the required level of intensity, or in a complete refusal to continue this exercise. Restoration of functions to the original, pre-working level characterizes the state of the body for a certain time after stopping the exercise. Each of these periods in the state of the body is characterized by special dynamics of the physiological functions of various systems, organs and the entire organism as a whole. The presence of these periods, their characteristics and duration are determined primarily by the nature, intensity and duration of the exercise performed, the conditions for its implementation, as well as the degree of training of the athlete.
Question 38. Pre-launch state. It is known that before upcoming competitions and other emotional events, such as exams, a person experiences a special state. For some it is expressed in increased excitability and activity, for others - in low mood, lethargy, and isolation. This state is called pre-launch. In a trained athlete, it characterizes the restructuring of the body, strengthening its functions to perform the upcoming work. The pre-launch state in this case creates favorable conditions for the transition from rest to a high level of performance. In this case, there is an increase in body temperature by 0.5-1.5 degrees, an increase in the pulse rate by 1.5 times, increased and deepening of breathing, and an increase in blood pressure. The athlete is collected, smart, focused. In some easily excitable In athletes, the pre-start state can appear long (2-3 days) before the competition and is accompanied by excessive excitement, sometimes giving way to apathy - the so-called start fever occurs. It can negatively affect the athlete's functional capabilities. To prevent “starter fever”, you need to accustom yourself to the upcoming competitions through estimation, create favorable conditions for the regime, and eliminate everything that can cause increased excitability. Directly at the competition site, such persons should not watch the performances, but relax, being in a bright, warm, comfortable room, calmly talking with a coach or doctor. A warm shower, a soothing massage, and self-massage work well for excited people, and for apathy, stimulants are needed: a short cool shower, an energetic massage, a cup of coffee or strong tea, and in some cases, medications on the advice of a doctor.
Question 39. General warm-up nonspecific. It is aimed at increasing the functional state of the body and creating optimal excitation of the central and peripheral parts of the motor system. Even before work begins, conditions are created for the formation of new motor skills and the best manifestation of physical qualities. Warming up the muscles reduces their viscosity, increases the flexibility of the joint-motor system, promotes the release of oxygen from blood oxyhemoglobin to tissues, activates enzymes and accelerates the course of biochemical reactions. However, the warm-up should not lead the athlete to fatigue and cause a temperature increase above 380 C, which will cause a negative effect. Special part of the warm-up provides specific preparation for the upcoming work of precisely those nerve centers and skeletal muscles that bear the main load. The working dominants and the motor dynamic stereotypes created on their basis are revived, vegetative shifts reach the level necessary for rapid entry into work. The optimal duration of the warm-up is 10–30 minutes, and the interval before work should not exceed 15 minutes, after which the effect of the warm-up decreases. Periods of rest and work are characterized by a relatively stable state of body functions, with their well-functioning regulation. Between them there are 2 transition periods - working-in (from rest to work) and recovery (from work to rest). The period of working-in is counted from the start of work until a stable state appears. During running-in, 2 processes are carried out: transition of the body to the working level; attunement of various functions. First, motor functions are developed very quickly, and then more inert vegetative ones. Of the vegetative indicators, frequency parameters - heart rate and respiration rate - increase most quickly to the working level, then volumetric characteristics - stroke and minute blood volumes, inspiratory depth and minute respiration volume. The inertia of vegetative shifts is associated, in particular, with the fact that in the initial moments of work a powerful motor dominant has a negative effect on the vegetative centers. Run-in period may result in the appearance of a “dead point”. It occurs in insufficiently trained athletes as a result of incoordination of motor and autonomic functions. With too intense movements and a slow restructuring of vegetative processes, a noticeable oxygen debt increases, and a severe subjective state arises. With prolonged cyclic work of relatively constant power, a stable state arises in the athlete’s body, which lasts from the moment the work is completed until the onset of fatigue.
Question
The run-in period is counted from the start of operation until a stable state appears. During training, 2 processes are carried out: the body transitions to a working level; attunement of various functions. First, motor functions are developed very quickly, and then, more inert vegetative ones. Of the vegetative indicators, frequency parameters - heart rate and respiration rate - increase most quickly to the working level, then volumetric characteristics - stroke and minute blood volumes, inspiratory depth and minute respiration volume. The inertia of vegetative shifts is associated, in particular, with the fact that in the initial moments of work a powerful motor dominant has a negative effect on the vegetative centers. The run-in period may end with the appearance of a “dead point”. It occurs in insufficiently trained athletes as a result of incoordination of motor and autonomic functions. With too intense movements and a slow restructuring of vegetative processes, a noticeable oxygen debt increases, and a severe subjective state arises. With prolonged cyclic work of relatively constant power, a stable state arises in the athlete’s body, which lasts from the moment the work is completed until the onset of fatigue.
41 questions “Dead spot” During middle and long distance running, swimming, rowing, skiing and cycling, an athlete may experience a state of acute fatigue - a “dead point”. It will be expressed in a sharp decrease in performance, a feeling of tightness in the chest, suffocation, and muscle pain. Movements become slow, there is a desire to stop running, competition, coordination and attention are impaired; neuropsychic activity declines, and the will to win sharply decreases. At the same time, breathing becomes rapid and shallow, the pulse is frequent, and blood pressure is increased. In this case, the athlete must, through an effort of will, force himself to continue moving, competing, working, and then the “dead point” is replaced by a state of relief - a “second wind” sets in. Breathing becomes rarer, deeper, more rhythmic, the feeling of heaviness in the muscles decreases, and performance increases. Sweating, which began during the “dead point”, becomes profuse by the onset of the “second wind”. The emergence of a “dead point” is explained by the fact that that intense muscle load in an athlete begins immediately after the start, and the activity of the respiratory and circulatory organs develops gradually and reaches a high level after 3-5 minutes. Consequently, there is a violation of consistency in the activity of the central nervous system, internal organs and motor system. Overcoming this condition leads to the appearance of a “second wind”. To prevent a “dead spot”, an intensive warm-up before the start and a gradual increase in the pace of movement are necessary. It is recommended to take 50 grams of glucose with fruit juice 12-20 minutes before the start. What matters in overcoming the “dead spot” is the encouragement of your comrades and coach. The “dead point” during running occurs at different intensity voltages over different distances and time (see table).
Question 42. Based on the nature of oxygen supply to the body, 2 types of steady state have been identified: an apparent (false) steady state when an athlete reaches the level of maximum oxygen consumption, but this consumption does not cover the high oxygen demand and a significant oxygen debt is formed; a true steady state when working at moderate power, when oxygen consumption corresponds to the oxygen demand, and almost no oxygen debt is formed .With the exception of short-term cyclic exercises of maximum power, a steady state is established in all other power zones after the end of the run-in. At the same time, the operating power, despite some deviations, is almost constant. This condition is characterized by the following features: 1.mobilization of all body systems to a high operating level;2 stabilization of many indicators that affect sports performance - length and frequency of steps, amplitude of oscillations of the general center of mass, frequency and depth of breathing, heart rate, level of oxygen consumption, etc.;3 coordination the work of various body systems, which replaces their discoordination of the working-in period - for example, a certain ratio of the rate of breathing and movement is established. Various types of standard acyclic exercises, as well as situational exercises, are characterized by variable power of work, i.e. absence of classical forms of steady state. Performing various exercises in gymnastics, diving, weightlifting, throwing, long jump, high jump, pole jumping, shooting, etc. very short-lived. Unlike long-term cyclic exercises, it is impossible to achieve a steady state in terms of oxygen consumption and other physiological indicators. However, repeated work in these sports causes a peculiar manifestation of the process of development and subsequent stabilization of functions. Each previous exercise serves as a warm-up for the next one and causes the body to work on it with a gradual increase in functional shifts up to the required working level with increased efficiency. In sports games and martial arts, the activity of an athlete is characterized not only by a change in the current situation, but also by a variable power of work. Despite the constant changes in power, after running in, various somatic and vegetative indicators are established within a certain optimal operating range. Maintaining this optimal range of functionality requires the necessary expenditure of energy and voluntary effort. Each athlete has an individual duration of continuous preservation of this state. The optimal dose of continuous work depends on congenital characteristics, level of sportsmanship, technical or tactical focus of the training session, intensity of activity, and other reasons. Fencers, for example, use various micro-pauses to restore some body functions. These pauses should not be long, so as not to reduce the achieved operating level. But these pauses allow you to avoid the rapid onset of fatigue, maintain a high level of attention, and somewhat restore motor and autonomic functions.
Question 43. Characteristics of fatigue. Good health is the result of chemical processes that establish a constant balance between poisons and antidotes in our body. When overworked, there is an excessive release of toxic substances into the body (for example, lactic acid), which suppress the activity of our defenses and, therefore, disrupt this natural balance. It has been found that as a result of this, the medulla and adrenal cortex reduce the secretion of adrenaline and hormones that ensure normal chemical balance in the body. Fatigue is a natural reaction of the body that requires rest and sleep after performing physical or mental work. Prolonged fatigue is a pathological condition that causes various dysfunctions of the body and is accompanied by a feeling of malaise, apathy or increased nervousness. These alarming symptoms indicate that our body is depressed by overwork, does not get enough rest, or is weakened by illness, mental trauma, various overexertion or stress. Fatigue turns into neurasthenia. At this stage, a tired body can no longer regain its strength through rest alone. In our brain there are regulatory nerve centers that, in a state of wakefulness, group, direct and coordinate all nerve impulses. The network of these centers is closely connected with the hypothalamus, which registers and directs our emotions, influences moods, attachments, instincts, exercises indirect control of all functions of our body, provides, if necessary, our protection and allows us to restore our strength during sleep, which interrupts connections , sometimes very complex and stormy, between the processes of excitation and inhibition. Any overwork, mental or physical, any impact, external or internal, on our nervous system is reflected in these centers, and a moment comes when they are unable to perform their functions. “Overfatigue diseases” are approaching us. If you are tired for a long time beyond the permissible limit and do not have the opportunity to restore your strength, this leads to the fact that the “control panel”, located, as we already know, in the brain , begins to send commands that exceed the actual capabilities of your muscles, and their execution requires an ever-increasing amount of effort. You feel very tired, but since you need to carry out the planned program, finish certain work on time, you overcome yourself, and as a result, your nervous system, without any interference from consciousness, more and more often sends persistent orders that require reduce the duration of breaks. Your tired muscles contract sharply and stiffen.. In a state of rest, convulsions often occur. This deep fatigue is never a local process. It spreads to nerve cells, which underlie all body functions, and disrupts the functioning of nerve centers and endocrine glands. The machine works irregularly, and it malfunctions more and more often, because there has been a mismatch in the entire natural defense system and a disruption in the rhythm of inner life. The vicious circle has closed. If you are nervously overtired, the orders given by your brain will not be proportional to the effort required, and you will become physically exhausted. Physical fatigue, if it has not yet led to complete exhaustion of strength, it is much easier to heal than mental fatigue, the nature of which is very complex and consists of many internal and external factors.
Question 44. Fatigue, as a predisposing factor (risk factor), is noted in 20% of cases of the development of neuroses (neurasthenia) in children and adults. For the occurrence of neurosis and exhaustion of the nervous system, it is necessary to be accompanied by violations of the work and rest regime, the dominance of negative emotions in a person’s state of mind. Exhaustion neurasthenia occurs in 2.8% of students from among those who presented asthenic complaints. The younger the child, the less often he may experience exhaustion neurosis. Many experts do not recognize the occurrence of true exhaustion of the nervous system in childhood. I. P. Pavlov said that “mental tension is quite difficult work.” It is accompanied by an increase in the tone of cerebral vessels, their narrowing, disruption of blood supply to the brain, nutrition of nerve cells, which leads to the development of fatigue. There are acute and chronic fatigue. P They are the first to understand the feeling of fatigue, accompanied by psychophysiological changes in the body that occur as a result of work. Subjectively experienced fatigue and lethargy are accompanied by a decrease in performance. The student is more often distracted from classes, his head becomes heavy, and yawning appears. Sometimes headaches occur. Blood pressure rises and pulse quickens. As a rule, students feel tired from studying on the way home, in the fresh air. Psychophysiological changes return to normal levels within 24 hours. Therefore, acute fatigue should be considered as a physiologically protective reaction of the body to any load. You should not be afraid of acute fatigue. Developing endurance in any activity, physical or mental, necessarily requires experiencing a state of fatigue and fatigue. You should not be afraid of fatigue, but of overwork (chronic fatigue). With it, restoration of psychophysiological parameters does not occur during the day, and night sleep does not help either. Scientific research has established that changes in cerebral circulation depend not so much on the duration of work, but on its nature, neuro-emotional tension, responsibility for its correct implementation, i.e., on many psychological factors. At the end of the 2nd quarter, 40% of students in special schools (language, mathematics) showed a state of overwork, which was explained, first of all, by improper organization of work and rest. Chronic fatigue can be considered as a pre-morbid state. Foci of stagnant inhibition of the cerebral cortex explain the well-known phenomena of “getting stuck” on the same thought, returning the eyes to a line that has already been read . Against the background of chronic Fatigue results in irritability and an unhealthy, not cheerful, not active state of excitement, inherent in childhood and primary school age. New acute fatigue can accumulate. This leads to asthenic reactions, and if preventive measures are not taken, asthenic syndrome occurs.
Question 45. Physiological characteristics of recovery processes. Recovery processes- the most important link in an athlete’s performance. The ability to recover during muscle activity is a natural property of the body, which significantly determines its trainability. Therefore, the speed and nature of recovery of various functions after physical activity are one of the criteria for assessing the functional readiness of athletes. 1. GENERAL CHARACTERISTICS OF RESTORATION PROCESSES During muscular activity, anabolic and catabolic processes associated with each other occur in the body of athletes, with dissimilation prevailing over assimilation. In accordance with the concept of Academician V.A. Engelhardt (1953), any splitting reaction causes or intensifies resynthesis reactions in the body, which, after cessation of labor activity, lead to the predominance of assimilation processes. At this time, energy resources expended during training and competitive work are replenished, oxygen debt is eliminated, decay products are removed, neuroendocrine, animal and autonomic systems are normalized, and homeostasis is stabilized. The entire set of physiological, biochemical and structural changes occurring during this period, which ensure the transition of the body from the working level to the initial (pre-working) state, is united by the concept of restoration. When characterizing restoration processes, one should proceed from the teachings of I.P. Pavlov that the processes of exhaustion and restoration in the body (active organ) are closely related to each other and to the processes of excitation and inhibition in the central nervous system. This position is fully confirmed by the experimental studies of G.V. Folbort (1951), in which a close connection was established between the processes of depletion and restoration of functional potentials in a working organ. It has also been shown that the greater the energy expenditure during work, the more intense the processes of their recovery. But if the depletion of functional potentials during work exceeds the optimal level, then complete recovery does not occur. In this case, physical activity causes further inhibition of cellular anabolism processes. If renewal reactions in cells do not correspond to catabolic processes in the body, structural changes can occur, leading to dysfunction and even damage to cells. After the end of physical activity, the human body retains functional changes inherent in the period of sports activity for some time, and only then the main recovery processes begin to take place. , which are heterogeneous in nature. It is important to emphasize that as a result of functional and structural changes that take place during the recovery process, the body’s functional reserves expand, and super-recovery (supercompensation) occurs. The processes of restoration of various functions in the body can be divided into three separate periods. The first (working) period includes those recovery reactions that are carried out during the process of muscle work itself (recovery of ATP, creatine phosphate, the transition of glycogen into glucose and the resynthesis of glucose from its breakdown products - gluconeogenesis). Working recovery maintains the normal functional state of the body and acceptable parameters of the main homeostatic constants in the process of performing a muscle load. Working recovery has a different genesis depending on the intensity of muscle work. When performing a moderate load, the supply of oxygen to working muscles and organs covers the body’s oxygen demand, and ATP resynthesis occurs aerobically. Recovery in these cases occurs at an optimal level of redox processes. Such conditions are observed during low-intensity training loads, as well as during portions of long-distance running, which is characterized by a true steady state. However, during acceleration, as well as in the “dead point” state, aerobic resynthesis is supplemented by anaerobic metabolism. Second (early) recovery period observed immediately after the end of light and moderate work for several tens of minutes and is characterized by the restoration of a number of already mentioned indicators, as well as the normalization of oxygen debt, glycogen, and some physiological, biochemical and psychophysiological constants.
Question 46. Fatigue during physical and mental work. Recovery. Any muscular activity, physical exercise, or sports increase the activity of metabolic processes, train and maintain at a high level the mechanisms that carry out metabolism and energy in the body, which has a positive effect on a person’s mental and physical performance. However, with an increase in physical or mental stress, the amount of information, as well as the intensification of many types of activity, a special condition called fatigue develops in the body. Fatigue - this is a functional state that temporarily arises under the influence of prolonged and intense work and leads to a decrease in its effectiveness. Fatigue is manifested in the fact that muscle strength and endurance decreases, coordination of movements worsens, energy costs increase when performing work of the same nature, the speed of information processing slows down, memory deteriorates, the process of concentrating and switching attention, assimilation of theoretical material becomes difficult. Fatigue is associated with a feeling of tiredness, and at the same time it serves as a natural signal of possible exhaustion of the body and a protective biological mechanism that protects it from overexertion. Fatigue that occurs during exercise is It is also a stimulant that mobilizes both the reserves of the body, its organs and systems, and recovery processes. Fatigue occurs during physical and mental activity. It can be acute, i.e. manifest itself in a short period of time, and chronic, i.e. be of a long-term nature (up to several months); general, i.e. characterizing changes in the functions of the body as a whole, and local, affecting any limited muscle group, organ, analyzer. There are two phases of fatigue: compensated (when there is no obvious decrease in performance due to the fact that the body’s reserve capacities are activated) and uncompensated (when the body’s reserve capacities are exhausted and performance is clearly reduced). Systematic performance of work against the background of under-recovery, ill-conceived work organization, excessive neuropsychic and physical stress can lead to overwork, and consequently to overstrain of the nervous system, exacerbations of cardiovascular diseases, hypertension and peptic ulcers, and a decrease in the body’s protective properties. The physiological basis of all these phenomena is an imbalance of excitatory-inhibitory nervous processes. Mental fatigue is especially dangerous for a person’s mental health; it is associated with the ability of the central nervous system to work under overload for a long time, and this can ultimately lead to the development of extreme inhibition and disruption of the coherence of the interaction of autonomic functions. It is possible to eliminate fatigue, increasing the level of general and specialized fitness of the body, optimizing its physical, mental and emotional activity. Recovery- a process occurring in the body after cessation of work and consisting in a gradual transition of physiological and biochemical functions to the original state. The time during which the physiological status is restored after performing a certain job is called the recovery period. It should be remembered that in the body, both during work and in pre-work and post-work rest, at all levels of its vital activity, interconnected processes of consumption and restoration of functional, structural and regulatory reserves continuously occur. During work, the processes of dissimilation prevail over assimilation, and the more, the greater the intensity of the work and the less readiness of the body to perform it. In the recovery period, assimilation processes predominate, and the restoration of energy resources occurs in excess of the initial level (super-recovery, or super-compensation). This is of great importance for increasing the fitness of the body and its physiological systems, ensuring increased performance. Schematically, the recovery process can be represented in the form of three complementary links: 1) elimination of changes and disturbances in neurohumoral regulation systems; 2) removal of decay products formed in the tissues and cells of the working organ from the places of their origin; 3) elimination of decay products from the internal environment of the body. Throughout life, the functional state of the body changes periodically. Such periodic changes may occur at short intervals or over long periods. Periodic recovery is associated with biorhythms, which are determined by daily periodicity, time of year, age-related changes, gender characteristics, the influence of natural conditions, and the environment. Thus, changes in time zone, temperature conditions, and geomagnetic storms can reduce recovery activity and limit mental and physical performance. Distinguish between early and late recovery phases. The early phase ends a few minutes after light work, after hard work - after a few hours; late recovery phases can last up to several days. Fatigue is accompanied a phase of reduced performance, and after some time it may be replaced by a phase of increased performance. The duration of these phases depends on the degree of training of the body, as well as on the work performed. The functions of various body systems are restored not at the same time. For example, after a long run, the external respiration function (frequency and depth) is the first to return to its original parameters; after a few hours, heart rate and blood pressure stabilize; indicators of sensorimotor reactions return to the original level after a day or more; In marathon runners, the basal metabolism is restored three days after the race. A rational combination of stress and rest is necessary in order to maintain and develop the activity of recovery processes. Additional means of recovery can be factors of hygiene, nutrition, massage, biologically active substances (vitamins). The main criterion for the positive dynamics of recovery processes is readiness for repeated activities. and the most objective indicator of recovery is the maximum volume of repeated work. Particular care must be taken into account the nuances of recovery processes when organizing physical exercises and planning training loads. It is advisable to perform repeated loads in the phase of increased performance. Too long rest intervals reduce the effectiveness of the training process. Thus, after a speed run of 60-80 m, the oxygen debt is eliminated within 5-8 minutes. The excitability of the central nervous system remains at a high level during this time. Therefore, an interval of 5-8 minutes will be optimal for repeating speed work. To speed up the recovery process, active rest is used in sports practice, i.e. switching to another type of activity. The importance of active rest for restoring performance was first established by the Russian physiologist I.M. Sechenov (1829-1905). He showed, for example, that a tired limb recovers quickly not with passive rest, but with work with another limb.
According to the program developed by the International Committee for the Standardization of Physical Readiness Tests, the determination of performance should take place in four areas:
1. medical examination;
2. determination of physiological reactions of different body systems to physical activity;
3. determination of physique and body composition in correlation with physical performance;
4. determination of the ability to perform physical activity and movements in a set of exercises, the implementation of which depends on different body systems.
The purpose of testing during physical education and sports is to assess the functional state of the body systems and the level of physical performance (fitness).
Testing should be understood as the reaction of individual systems and organs to certain influences (the nature, type and severity of this reaction). Evaluation of test results can be both qualitative and quantitative.
To assess the functional state of the body, various functional tests can be used.
1. Tests with dosed physical activity: one-, two-, three- and four-moment.
2. Tests with changes in body position in space: orthostatic, clinostatic, clinoorthostatic.
3. Tests with changes in intrathoracic and intra-abdominal pressure: straining test (Valsalva).
4. Hypoxemic tests: tests with inhalation of mixtures containing different ratios of oxygen and carbon dioxide, breath holding and others.
5. Pharmacological, nutritional, temperature, etc.
In addition to these functional tests, specific tests are also used with a load characteristic of each type of motor activity.
Physical performance is an integral indicator that allows one to judge the functional state of various body systems and, first of all, the performance of the circulatory and respiratory apparatus. It is directly proportional to the amount of external mechanical work performed at high intensity.
To determine the level of physical performance, tests with maximum and submaximal load can be used: maximum oxygen consumption (VO2), PWC170, Harvard step test, etc.
1. Determination of the level of physical performance using the PWC170 test
For work you need: a bicycle ergometer (or a step, or a treadmill), a stopwatch, a metronome.
The PWC170 test is based on the principle that there is a linear relationship between heart rate (HR) and exercise power. This allows you to determine the amount of mechanical work at which the heart rate reaches 170, by constructing a graph and linear extrapolation of the data, or by calculating using the formula proposed by V. L. Karpman. A heart rate equal to 170 beats per minute corresponds to the beginning of the zone of optimal functioning of the cardiorespiratory system. In addition, this heart rate disrupts the linear nature of the relationship between heart rate and physical work power.
The load can be performed on a bicycle ergometer, on a step (step test), or as specific for a particular sport.
Option No. 1 (with a bicycle ergometer).
The subject performs two loads sequentially for 5 minutes. with a 3-minute rest interval in between. In the last 30 sec. In the fifth minute of each load, the pulse is calculated (by palpation or electrocardiographic method).
The power of the first load (N1) is selected according to the table depending on the body weight of the subject so that at the end of the 5th minute the pulse (f1) reaches 110...115 beats/min.
The power of the second (N2) load is determined according to table. 7 depending on the value of N1. If the N2 value is correctly selected, then at the end of the fifth minute the pulse (f2) should be 135...150 beats/min.
Table: Approximate second load power values recommended when determining PWC170
|
Operating power at first load, kgm/min |
Power, kgm/min (N2) |
||||
|
Heart rate N1 beats/min |
|||||
To accurately determine N2, you can use the formula:
N2 = N1
where N1 is the power of the first load,
N2 - power of the second load,
f1 - heart rate at the end of the first load,
f2 - heart rate at the end of the second load.
Then PWC170 is calculated using the formula:
PWC170 = N1 + (N2 - N1) [(170 - f1) / (f2 - f1)]
The value of PWC170 can be determined graphically (Fig. 3).
To increase objectivity in assessing the power of work performed at a heart rate of 170 beats/min, the influence of the weight indicator should be excluded, which is possible by determining the relative value of PWC170. The PWC170 value is divided by the weight of the subject, compared with a similar value for the sport (Table 8), and recommendations are given.
Figure Determination of physical performance using the PWC170 test using graphical extrapolation
Option No. 2. Determining the value of PWC170 using a step test.
The principle of operation is the same as in work No. 1. The speed of climbing a step when performing the first load is 3...12 ascents per minute, with the second - 20...25 ascents per minute. Each ascent is made in 4 counts per step 40-45 cm high: for 2 counts of ascent and for the next 2 counts - descent. 1st load - 40 steps per minute, 2nd load 90 (the metronome is set to these numbers).
The pulse is calculated for 10 seconds, at the end of each 5-minute load.
The power of the loads performed is determined by the formula:
N = 1.3 h n P,
where h is the height of the step in m, n is the number of ascents per minute,
P - body weight. of the subject in kg, 1.3 - coefficient.
Then the value of PWC170 is calculated using the formula (see option No. 1).
Option No. 3. Determining the value of PWC170 under specific loads (for example, running).
To determine physical performance according to the PWC170 (V) test with specific loads, it is necessary to register two indicators: movement speed (V) and heart rate (f).
To determine the speed of movement, you need to use a stopwatch to accurately record the length of the distance (S in m) and the duration of each physical activity (f in sec.)
where V is the speed of movement in m/s.
The heart rate is determined during the first 5 seconds. recovery period after running using palpation or auscultation method.
The first race is performed at a “jogging” pace at a speed equal to 1/4 of the maximum possible for a given athlete (approximately every 100 m for 30-40 seconds).
After a 5-minute rest, the second load is performed at a speed equal to 3/4 of the maximum, i.e. in 20-30 seconds. every 100 m.
Distance length 800-1500 m.
PWC170 is calculated using the formula:
PWC170 (V) = V1 + (V2 - V1) [(170 - f1) / (f2 - f1)]
where V1 and V2 are the speed in m/s,
f1 and f2 - heart rate after which race.
2. Determination of maximum oxygen consumption (MOC)
MPC expresses the maximum “throughput” capacity of the oxygen transport system for a given person and depends on gender, age, physical fitness and body condition.
On average, MOC in people with different physical conditions reaches 2.5...4.5 l/min, in cyclic sports - 4.5...6.5 l/min.
Methods for determining MIC: direct and indirect. The direct method for determining MOC is based on the athlete performing a load whose intensity is equal to or greater than his critical power. It is unsafe for the person being examined, as it is associated with extreme stress on the body’s functions. More often they use indirect methods of determination, based on indirect calculations and the use of low load power. Indirect methods for determining MIC include the Astrand method; determination using the Dobeln formula; by size PWC170, etc.
Option No. 1. Determination of MIC using the Astrand method.
For work you need: bicycle ergometer, steps 40 cm and 33 cm high, metronome, stopwatch, Astrand nomogram.
On a bicycle ergometer, the subject performs a 5-minute load of a certain power. The load value is selected so that the pulse rate at the end of work reaches 140-160 beats/min (approximately 1000-1200 kgm/min). The pulse is counted at the end of the 5th minute for 10 seconds. palpation, auscultation or electrocardiographic method. Then, using the Astrand nomogram (Fig. 4), the MIC value is determined, for which, by connecting the heart rate during exercise (scale on the left) and the body weight of the subject (scale on the right), the MOC value is found at the point of intersection with the central scale.

Option No. 2. Determination of MIC using a step test.
Within 5 minutes, the subject climbs a step 40 cm high for men and 33 cm high for women at a speed of 25.5 cycles per minute. The metronome is set to frequency 90.
At the end of the 5th minute for 10 seconds. Pulse rate is recorded. The IPC value is determined using the Astrand nomogram and compared with the standard for sports specialization. Considering that MIC depends on body weight, calculate the relative value of MIC (MIC/weight) and compare with average data, write a conclusion and make recommendations.
Option No. 3. Determination of MIC by PWC170 value.
The MIC is calculated using the formulas proposed by V.L. Karpman:
MPC = 2.2 PWC170 + 1240
For athletes specializing in speed-strength sports;
MPC = 2.2 PWC170 + 1070
For endurance athletes.
Option No. 4. Determination of performance using the Cooper test
The Cooper test consists of running the maximum possible distance on level ground (stadium) in 12 minutes.
If signs of fatigue occur (severe shortness of breath, tachyarrhythmia, dizziness, heart pain, etc.), the test is stopped.
The test results correspond to the MOC value determined on the treadmill.
The Cooper test can be used when selecting schoolchildren in sections for cyclic sports, during training to assess the state of fitness.

Option No. 5. Novakki test (maximum test).
Purpose: to determine the time during which the subject is able to perform work with maximum effort.
Required equipment: bicycle ergometer, stopwatch.
The subject performs a load on a bicycle ergometer at the rate of 1 W/kg for 2 minutes. Every 2 minutes the load increases by 1 W/kg until the maximum value is reached.
Evaluation of the result. High performance according to this test corresponds to a value of 6 W/kg, when performed for 1 minute. A good result corresponds to a value of 4-5 W/kg for 1-2 minutes.
This test can be used for trained persons (including in youth sports), for untrained persons and persons in the period of convalescence after illness. In the latter case, the initial load is set at the rate of 0.25 W/kg.
3. Determination of the level of physical performance according to the Harvard Step Test (HST)
Physical performance is assessed by the value of the GST index (IGST) and is based on the rate of heart rate recovery after climbing a step.
For work you need: steps of various heights, a metronome, a stopwatch.
Next, the subject performs 10-12 squats (warm-up), after which he begins to climb the step at a speed of 30 cycles per minute. The metronome is set to a frequency of 120 beats/min, the rise and fall consists of 4 movements, each of which will correspond to a metronome beat: for 2 beats - 2 steps of rise, for 2 beats - 2 steps of descent.
Ascent and descent always start from the same foot.
If the subject lags behind the rhythm for 20 seconds due to fatigue, testing is stopped and the time spent working at the given pace is recorded.
Table Height of steps and time of ascent depending on gender and age (according to I. Aulik)

Note. S denotes the surface of the subject’s body (m2) and is determined by the formula:
S = 1 + (P ± DH) / 100
where S is the surface of the body; P - body weight;
DN - deviation of the subject's height from 160 cm with the corresponding sign.
After finishing work within 1 minute. During the recovery period, the subject sits and rests. Starting from the 2nd minute of the recovery period, in the first 30 seconds. At 2, 3 and 4 minutes the pulse is measured.
IGST is calculated using the formula:
IGST = (t 100) / [(f1 + f2 + f3) 2]
where t is the duration of the ascent, in seconds.
f1, f2, f3 - heart rate, for 30 seconds. at 2, 3 and 4 minutes of the recovery period, respectively.
In the case when the subject stops climbing prematurely due to fatigue, the IGST is calculated using the abbreviated formula:
IGST = (t 100) / (f1 5.5)
where t is the test execution time, in seconds,
f1 - heart rate for 30 seconds. at the 2nd minute of the recovery period.
With a large number of subjects, the table can be used to determine IGST. 12, 13, for which the sum of three pulse counts (f1 + f2 + f3) in tens is found in the vertical column (tens), in the upper horizontal line - the last digit of the sum and at the intersection - the IGST value. Then physical performance is assessed using standards (score tables).
Determination of IGST using the abbreviated formula in adult men

4. Modified orthostatic test
Purpose: to assess the state of orthostatic stability of the body.
The orthostatic test is used to identify the state of latent orthostatic instability and to monitor the dynamics of the state of fitness in complex coordination sports. The sample is based on. that when moving from a horizontal to a vertical position, due to a change in hydrostatic conditions, the primary venous return of blood to the right side of the heart decreases, resulting in an underload of the heart with volume and a decrease in systolic blood volume. To maintain the minute blood volume at the proper level, the heart rate reflexively increases (by 5-15 beats per minute).
In pathological conditions, overtraining, overexertion, after infectious diseases, or in congenital orthostatic instability, the depository role of the venous system turns out to be so significant that a change in body position leads to dizziness, darkening of the eyes, even fainting. Under these conditions, the compensatory increase in heart rate is insufficient, although it is significant.
For work you need: a couch, a sphygmomanometer, a phonendoscope, a stopwatch.
Compare the results with the recommended ones, develop ways to optimize orthostatic stability using physical education. After a preliminary rest for 5 minutes. in a lying position, heart rate is determined 2-3 times and blood pressure is measured. Then the subject slowly stands up and remains in an upright position for 10 minutes. in a relaxed position. To ensure the best relaxation of the leg muscles, it is necessary to step back one foot from the wall, lean your back against it, and place a cushion under the sacrum. Immediately after moving to a vertical position for the entire 10 minutes. at every minute, heart rate and blood pressure are recorded (for the first 10 s - heart rate, for the remaining 50 s - blood pressure).
The state of orthostatic stability is assessed using the following indicators:
1. Heart rate difference, at 1st minute. and at the 10th minute. in relation to the initial value in the supine position. Blood pressure increases by 10-15%.
2. Heart rate stabilization time.
3. The nature of changes in blood pressure in a standing position.
4. Well-being and severity of somatic disorders (pallor of the face, darkening of the eyes, etc.).
Satisfactory orthostatic stability:
1. The increase in heart rate is small and in the 1st minute. orthoposition ranges from 5 to 15 beats/min., at the 10th min. does not exceed 15-30 beats/min.
2. Stabilization of the pulse occurs within 4-5 minutes.
3. Systolic blood pressure remains unchanged or decreases slightly, diastolic blood pressure increases by 10-15% relative to its value in a horizontal position.
4. Feeling good and there are no signs of somatic disorder.
Signs of orthostatic instability are an increase in heart rate by more than 15-30 beats/min, a pronounced drop in blood pressure and vegetosomatic disorders of varying severity.

5. Determination of the anaerobic capabilities of the body by the value of maximum anaerobic power (MAP)
Anaerobic capabilities (i.e., the ability to work in oxygen-free conditions) are determined by the energy generated during the breakdown of ATP, creatine phosphate and glycolysis (anaerobic breakdown of carbohydrates). The degree of adaptation of the body to work in oxygen-free conditions determines the amount of work that a person can perform in these conditions. This adaptation is important in developing the body's speed capabilities.
During mass examinations, R. Margaria’s test (1956) is used to determine MAM. The power of running up the stairs at maximum speed in a short time is determined.
Methodology. A staircase, approximately 5 m long, 2.6 m high, with an inclination of more than 30°, can be run in 5-6 seconds. (approximate time of maximum run).
The subject is located 1-2 m from the stairs and performs the test on command. The time is recorded in seconds. The height of the steps is measured, their number is counted, and the total height of the rise is determined:
MAM = (P h) / t kgm/s
where P is weight in kg, h is lifting height in m, t is time in sec.
Result assessment: the highest value of MAM is observed at 19-25 years old, from 30-40 years old it decreases. In children it tends to increase.
For untrained individuals, MAM is 60...80 kgm/s, for athletes - 80...100 kgm/s. To convert to watts, the resulting value must be multiplied by 9.8, and to convert to kilocalories per minute - by 0.14.
Testing the physical performance of persons involved in physical education and sports at rest does not reflect its functional state and reserve capabilities, since the pathology of an organ or its functional insufficiency manifests itself more noticeably under load conditions than at rest, when the requirements for it are minimal.
Unfortunately, the function of the heart, which plays a leading role in the life of the body, is in most cases assessed based on examination at rest. Although it is obvious that any violation of the pumping function of the heart is more likely to manifest itself at a minute volume of 12-15 l/min than at 5-6 l/min. In addition, insufficient reserve capabilities of the heart can only manifest themselves in work that exceeds the usual load in intensity. This also applies to hidden coronary insufficiency, which is often not diagnosed by ECG at rest.
Therefore, assessment of the functional state of the cardiovascular system at the modern level is impossible without the widespread use of stress tests.
Load test objectives:
1) determination of performance and suitability for practicing a particular sport;
2) assessment of the functional state of the cardiorespiratory system and its reserves;
3) forecasting probable sports results, as well as forecasting the likelihood of the occurrence of certain deviations in health status when undergoing physical activity;
4) identification and development of effective preventive and rehabilitation measures for highly qualified athletes;
5) assessment of the functional state and effectiveness of the use of rehabilitation means after injuries and diseases in training athletes.
Recovery tests
Recovery tests involve taking into account changes and determining the recovery time after standard physical activity in such indicators of the cardiorespiratory system as heart rate (HR), blood pressure (BP), electrocardiogram (EKG) readings, respiratory rate (RR) and many others.
In sports medicine, V.V. samples are used. Gorinevskgo (60 jumps for 30 s), Deshin and Kotov test (three-minute running in place at a pace of 180 steps per minute), Martinet test (20 squats) and other functional tests. When conducting each of these tests, heart rate and blood pressure are taken into account before the load and after its end at the 1st, 2nd, 3rd and 4th minutes.
Recovery tests also include various versions of the step-test.
In 1925, A. Master introduced a two-stage test, where heart rate and blood pressure were also recorded after a certain number of climbs up a standard step. Later, this test began to be used to record ECG after exercise (A. Master and H. Jafte, 1941). In its modern form, the two-step test provides for a certain number of climbs on a standard double step for 1.5 minutes, depending on the age, gender and body weight of the subject (see Table. ), or twice the number of rises in 3 minutes with a double test (the height of each step is 23 cm). An ECG is recorded before and after exercise.
Minimum number of lifts (times) per step depending on the weight,
age and gender at the Master's sample
| Body weight, kg | Age, years | ||||
| 20-29 | 30-39 | 40-49 | 50-59 | 60-69 | |
| number of ascents per step* | |||||
| 40-44 | 29 (28) | 28 (27) | 27 (24) | 25 (22) | 24 (21) |
| 45-49 | 28 (27) | 27 (25) | 26 (23) | 25 (22) | 23 (20) |
| 50-54 | 28 (26) | 27 (25) | 25 (23) | 24 (21) | 22 (19) |
| 55-59 | 27 (25) | 26 (24) | 25 (22) | 23 (20) | 22 (18) |
| 60-64 | 26 (24) | 26 (23) | 24 (21) | 23 (19) | 21 (18) |
| 65-69 | 25 (23) | 25 (21) | 23 (20) | 22 (19) | 20 (17) |
| 70-74 | 24 (22) | 24 (21) | 23 (19) | 21 (18) | 20 (16) |
| 75-79 | 24 (21) | 24 (20) | 22 (19) | 20 (17) | 19 (16) |
| 80-84 | 23 (20) | 23 (19) | 22 (18) | 20 (16) | 18 (15) |
| 85-89 | 22 (19) | 23 (18) | 21 (17) | 19 (16) | 18 (14) |
| 90-94 | 21 (18) | 22 (17) | 20 (16) | 19 (15) | 17 (14) |
| 95-99 | 21 (17) | 21 (15) | 20 (15) | 18 (14) | 16 (13) |
| 100-104 | 20 (16) | 21 (15) | 19 (14) | 17 (13) | 16 (12) |
| 105-109 | 19 (15) | 20 (14) | 18 (13) | 17 (13) | 15 (11) |
| 110-114 | 18 (14) | 20 (13) | 18 (13) | 16 (12) | 14 (11) |
* The number of lifts for women is given in parentheses.
Submaximal effort tests
Submaximal force tests are used in sports medicine to test elite athletes. Studies have shown that the most valuable information about the functional state of the cardiorespiratory system can be obtained by taking into account changes in the main hemodynamic parameters (indicators) not in the recovery period, but directly during the test. Therefore, an increase in loads is carried out until the limit of aerobic capacity (maximum oxygen consumption - MPK) is reached.
In sports medicine, submaximal load tests are also used, requiring 75% of the maximum tolerated load. They are recommended by WHO for widespread implementation (WHO Chronicle, 1971, 25/8, p. 380, etc.).
Various bicycle ergometers, treadmills, etc. are also used (Fig. ). If the age limits of the heart rate are exceeded (see table. Maximum permissible heart rate during an exercise test) it is advisable to stop the load.
Maximum permissible heart rate during an exercise test depending on age
In addition to exceeding the age limits of heart rate, the physical test should also be stopped in cases of clinical electrocardiographic signs indicating that the limit of exercise tolerance has been reached.
Clinical signs: 1) an attack of angina pectoris even in the absence of changes on the ECG; 2) severe shortness of breath; 3) great fatigue, pallor, coldness and dampness of the skin; 4) significant increase in blood pressure; 5) reduction in blood pressure by more than 25% from baseline; 6) refusal of the subject to continue the study due to discomfort.
Electrocardiographic signs: 1) the occurrence of frequent extrasystoles (4:40) and other pronounced rhythm disturbances; 2) violation of atrioventricular and intraventricular conduction; 3) horizontal or trough-shaped downward shift of the ST segment by more than 0.2 mV compared to the recording at rest; 4) elevation of the ST segment by more than 0.2 mV, accompanied by its descent in the opposite leads; 5) inversion, or the appearance of a pointed and raised T wave with an increase in amplitude by more than 3 times (or 0.5 mV) compared to the original in any of the leads (especially V 4); 6) a decrease in the amplitude of the R wave by at least 50% of its value at rest.
Harvard step test
The Harvard step test (L. broucha, 1943) consists of climbing a bench 50 cm high for men and 43 cm high for women for 5 minutes at a given pace. The rate of ascent is constant and equals 30 cycles per minute. Each cycle consists of four steps. The tempo is set by a metronome at 120 beats per minute. After completing the test, the subject sits on a chair and during the first 30 s, at the 2nd, 3rd and 4th minutes, the heart rate is calculated. If the subject falls behind the set pace during testing, the test is terminated.
An athlete’s physical performance is judged by the Harvard Step Test Index (HST), which is calculated based on the time to climb the step and heart rate after the end of the test. The height of the step and the time to climb it are selected depending on the gender and age of the subject (see table. Step height and ascent time in the Harvard step test).
Step height and ascent time in the Harvard step test
* Body surface can be determined using a nomogram for determining body surface by height and body weight for the article Assessment of physical development.
The Harvard Step Test Index is calculated using the formula:
IGST = (t x 100) / [(f 1 + f 2 + f 3) x 2]
where t is the ascent time in seconds, f 1, f 2, f 3 is the heart rate (HR) for 30 s at the 2nd, 3rd and 4th minutes of recovery, respectively.
For mass surveys, you can use the abbreviated formula:
IGST = (t x 100) / (f x 5.5)
where t is the ascent time in seconds, f is the heart rate (HR).
Counting is made easier when using see table. ; ; . Table Finding the index using the Harvard step test is intended for determining IGST in adults if the load was sustained to the end (that is, for 5 minutes). First, three pulse counts are summed up (f 1 + f 2 + f 3 = sum f), then the first two digits of this sum are found in the left vertical column, and the last digit is found in the top horizontal line. The required IGST is located at the intersection of the indicated lines. If the pulse was counted only once in an abbreviated form, then the IGST is found from the f 2 value of this count in a similar way in Table. Finding the index using the Harvard step test in abbreviated form. Table Dependence of IGST on ascent time facilitates the calculation of IGST with incomplete ascent time (short form).
Finding the index using the Harvard step test
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| 80 | 188 | 185 | 183 | 181 | 179 | 176 | 174 | 172 | 170 | 168 |
| 90 | 167 | 165 | 163 | 161 | 160 | 158 | 156 | 155 | 153 | 152 |
| 100 | 150 | 148 | 147 | 146 | 144 | 143 | 142 | 140 | 139 | 138 |
| 110 | 136 | 135 | 134 | 133 | 132 | 130 | 129 | 128 | 127 | 126 |
| 120 | 125 | 124 | 123 | 122 | 121 | 120 | 118 | 117 | 117 | 116 |
| 130 | 115 | 114 | 114 | 113 | 112 | 111 | 110 | 110 | 109 | 108 |
| 140 | 107 | 106 | 106 | 105 | 104 | 103 | 103 | 102 | 101 | 101 |
| 150 | 100 | 99 | 99 | 98 | 97 | 97 | 96 | 96 | 95 | 94 |
| 160 | 94 | 93 | 93 | 92 | 92 | 91 | 90 | 90 | 89 | 89 |
| 170 | 88 | 88 | 87 | 87 | 86 | 86 | 85 | 85 | 84 | 84 |
| 180 | 83 | 82 | 82 | 82 | 82 | 81 | 81 | 80 | 80 | 79 |
| 190 | 79 | 78 | 78 | 78 | 77 | 77 | 76 | 76 | 76 | 75 |
| 200 | 75 | 75 | 74 | 74 | 74 | 73 | 73 | 72 | 72 | 72 |
| 210 | 71 | 71 | 71 | 70 | 70 | 70 | 69 | 69 | 69 | 68 |
| 220 | 68 | 67 | 67 | 67 | 67 | 67 | 66 | 66 | 66 | 66 |
| 230 | 65 | 65 | 65 | 64 | 64 | 64 | 64 | 63 | 63 | 63 |
| 240 | 62 | 62 | 62 | 62 | 61 | 61 | 61 | 61 | 60 | 60 |
| 250 | 60 | 60 | 60 | 59 | 59 | 59 | 59 | 58 | 58 | 58 |
| 260 | 58 | 57 | 57 | 57 | 57 | 57 | 56 | 56 | 56 | 56 |
| 270 | 56 | 55 | 55 | 55 | 55 | 55 | 54 | 54 | 54 | 54 |
| 280 | 54 | 53 | 53 | 53 | 53 | 53 | 52 | 52 | 52 | 52 |
| 290 | 52 | 52 | 51 | 51 | 51 | 51 | 51 | 50 | 50 | 50 |
Table for finding the index according to the Harvard step test in full form in adults (t = 5 min)
Finding the index using the Harvard step test in abbreviated form
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| 30 | 182 | 176 | 171 | 165 | 160 | 156 | 152 | 147 | 144 | 140 |
| 40 | 136 | 133 | 130 | 127 | 124 | 121 | 119 | 116 | 114 | 111 |
| 50 | 109 | 107 | 105 | 103 | 101 | 99 | 97 | 96 | 94 | 92 |
| 60 | 91 | 89 | 88 | 87 | 85 | 84 | 83 | 81 | 80 | 79 |
| 70 | 78 | 77 | 76 | 75 | 74 | 73 | 72 | 71 | 70 | 69 |
| 80 | 68 | 67 | 67 | 66 | 65 | 64 | 63 | 63 | 62 | 61 |
| 90 | 61 | 60 | 59 | 59 | 58 | 57 | 57 | 56 | 56 | 55 |
| 100 | 55 | 54 | 53 | 53 | 52 | 52 | 51 | 51 | 50 | 50 |
| 110 | 50 | 49 | 49 | 48 | 48 | 47 | 47 | 47 | 46 | 46 |
Table for finding the index for the Harvard step test in abbreviated form for adults (t = 5 min)
Dependence of IGST on ascent time (short form)
| Pulse for the first 30 s from the 2nd minute of recovery | ||||||||
| Time, min | 40-44 | 45-49 | 50-54 | 55-59 | 60-64 | 65-69 | 70-74 | 75-79 |
| 0-0.1/2 | 6 | 6 | 5 | 5 | 4 | 4 | 4 | 4 |
| 0.1/2-1 | 19 | 17 | 16 | 14 | 13 | 12 | 11 | 11 |
| 1-1.1/2 | 32 | 29 | 26 | 24 | 22 | 20 | 19 | 18 |
| 1.1/2-2 | 45 | 41 | 28 | 24 | 21 | 29 | 27 | 25 |
| 2-2.1/2 | 58 | 52 | 47 | 43 | 40 | 36 | 34 | 32 |
| 2.1/2-3 | 71 | 64 | 58 | 53 | 48 | 45 | 42 | 39 |
| 3-3.1/2 | 84 | 75 | 68 | 62 | 57 | 53 | 49 | 46 |
| 3.1/2-4 | 97 | 87 | 79 | 72 | 66 | 61 | 57 | 53 |
| 4-4.1/2 | 110 | 98 | 89 | 82 | 75 | 70 | 65 | 61 |
| 4.1/2-5 | 123 | 110 | 100 | 91 | 84 | 77 | 72 | 68 |
| 5 | 129 | 116 | 105 | 96 | 88 | 82 | 77 | 71 |
In the left vertical column the actual ascent time is found (rounded to 30 s), and in the upper horizontal line - the number of pulse beats in the first 30 s from the 2nd minute of recovery.
Due to the high intensity of the load, the test is used only when examining athletes.
The criteria for assessing the results of the Harvard step test are given in table. Evaluation of the results of the Harvard step test.
Evaluation of the results of the Harvard step test
The highest figures (up to 170) were observed among elite athletes training for endurance (skiing, rowing, swimming, marathon running, etc.).
Submaximal stress tests
Submaximal stress tests are carried out with different types of loads:
1) immediately increase the load after warming up to the expected submaximal level for a given subject;
2) uniform load at a certain level with an increase in subsequent studies;
3) continuous or almost continuous increase in load;
4) stepwise increase in load;
5) stepwise increase in load, alternating with periods of rest. The first, third and fourth tests are used mainly when examining athletes, the second - for a comparative assessment of the tolerance of a certain load by any group of individuals. According to WHO recommendations, when examining healthy individuals, the initial load in women should be 150 kgm/min, followed by an increase to 300-450-600 kgm/min, etc.; for men - 300 kgm/min, followed by an increase to 600-900-1200 kgm/min, etc. The duration of each load stage is at least 4 minutes. Rest periods between load stages are 3-5 minutes.
Treadmill test (see Fig. ) usually starts at 6 km/h and then increases to 8 km/h, 10 km/h, etc. The movement slope increases stepwise to 2.5%.
Stress tests in children
Load tests in children under 10 years of age begin with minimal loads (up to 50 kgm/min), and from 10 years of age and older - taking into account body weight. Usually, as WHO recommends, from 100-150 kgm/min.
The easiest way to calibrate loads is on the scale of a bicycle ergometer. During a step test, the magnitude of the loads is determined based on the calculation of the weight of the subject, the height of the steps and the number of ascents on them. When testing with a treadmill, energy costs are calculated depending on the speed and slope (Fig. ).

Nomogram for determining total oxygen costs during the treadmill test (according to R. Shephard, 1969)
Taking into account the linear relationship between heart rate and the amount of oxygen consumption based on heart rate, one can judge the level of aerobic capacity of the subject during an exercise test and the level of load to achieve, for example, 75% of aerobic capacity (Table Approximate heart rate).
Approximate heart rate
| Aerobic capacity, % | Age, years | |||||||||
| 20-29 | 30-39 | 40-49 | 50-59 | 60-69 | ||||||
| Husband. | Women | Husband. | Women | Husband. | Women | Husband. | Women | Husband. | Women | |
| 40 | 115 | 122 | 115 | 120 | 115 | 117 | 111 | 113 | 110 | 112 |
| 60 | 141 | 148 | 138 | 143 | 136 | 138 | 131 | 134 | 127 | 130 |
| 75 | 161 | 167 | 156 | 160 | 152 | 154 | 145 | 145 | 140 | 142 |
| 100 | 195 | 198 | 187 | 189 | 178 | 179 | 170 | 171 | 162 | 163 |
Approximate heart rate (bpm) depending on aerobic capacity (according to R. Sheppard, 1969)
The table also gives an idea of the maximum heart rate in people of different genders and ages.
The maximum heart rate for people of different ages can be approximately determined by subtracting the number of years of the subject from 220. For example, for a person aged 30 years, the maximum heart rate is 220 - 30 = 190.
Submaximal Wahlund-Sjöstrand test
The Wahlund-Sjostrand submaximal test (W 170 or PWC 170) is recommended by WHO to determine physical performance upon reaching a heart rate of 170 beats/min (physical load power is expressed in kgm/min or W), at which the heart rate after exercise is set at 170 beats /min, that is W 170 (or PWC 170). This load level is the indicator of W 170.
For older age groups, taking into account the lower limit of permissible increase in heart rate, as well as for young athletes, the PWC 130 and PWC 150 tests are used - determining physical performance when the heart rate reaches 130 and 150 beats/min.
The test is performed as follows: the subject is subjected to two loads of different power (W 1 and W 2) on a bicycle ergometer for a duration of 5 minutes, each with 3 minutes of rest. The load is selected in such a way as to obtain several heart rate values in the range from 120 to 170 beats/min. At the end of each load, heart rate is determined (f 1 and f 2, respectively).
Based on the data obtained, graphs are constructed, where load power indicators (W 1 and W 2) are entered on the abscissa axis, and the corresponding heart rate is recorded on the ordinate axis (Fig. ). At the intersection of perpendiculars dropped to the corresponding points of the graph axes, coordinates 1 and 2 are found, a straight line is drawn through them until it intersects with the perpendicular restored from the heart rate point corresponding to 170 beats/min (coordinate 3). From it a perpendicular is lowered onto the abscissa axis, and thus the value of the load power is obtained at a heart rate equal to 170 beats/min.

PWC 170: f 1 and f 2 - heart rate at the first and second loads; W 1 and W 2 - power of the first and second loads
To simplify the calculation of operating power during the two-stage PWC 170 test, the following formula is recommended:
PWC 170 = x [(170 - f 1) / (f 1 - f 2)]
where PWC 170 is the power of physical activity at a heart rate of 170 beats/min, W1 and W2 are the power of the first and second loads (kgm/min or W); f 1 and f 2 - heart rate in the last minute of the first and second loads (in 1 min).
The following PWC 170 values in healthy people can be used as guidelines: for women - 422-900 kgm/min, for men - 850-1100 kgm/min. For athletes, this indicator depends on the type of sport and ranges from 1100-2100 kgm/min, and representatives of cyclic sports (rowing, road cycling, cross-country skiing, etc.) have even higher indicators. To compare similar individuals, the relative value of the PWC 170 indicator is calculated, for example, W/kg.
Determination of maximum oxygen consumption
Determination of maximum oxygen consumption (MOC). MPK is the main indicator of the productivity of the cardiorespiratory system. MPK is the largest amount of oxygen that a person is able to consume in one minute. MPK is a measure of aerobic power and an integral indicator of the state of the oxygen (O2) transport system. It is determined by an indirect or direct method.
The indirect method of measuring MPK is more often used (Fig. ), which does not require complex equipment. For the examination of highly qualified athletes, it is recommended to measure BMD using the direct method.

Graph for direct determination of maximum work and MPF based on submaximal exercise tests (after K. Lange Andersen and Smith-Siversten, 1966)
Normally, there is a linear relationship between the amount of oxygen consumption (OC) and heart rate.
MPK is the main indicator that reflects the functional capabilities of the cardiovascular and respiratory systems and physical condition in general, that is, aerobic capacity. This indicator (l/min, or more precisely, ml/min/kg) or its energy equivalent (kJ/min, kcal/min) is one of the leading indicators in the assessment and grading of a person’s physical condition. Thus, submaximal exercise tests, which provide information about aerobic capacity, are an essential tool for assessing the functional state of the body. The MPF value depends on the gender, age, and physical fitness of the subject and varies widely. Normal values for maximum oxygen consumption in school-age children and adults are given in Table. Maximum oxygen consumption in children and adolescents; Maximum oxygen consumption in adults.
Maximum oxygen consumption in children and adolescents
Maximum oxygen consumption in children and adolescents (according to J. Rutenfranz, T. Hettinger, 1959)
Maximum oxygen consumption (ml/min/kg) in adults
The subject is recommended to perform a bicycle ergometric load (the heart rate after cycling should be between (120-170 beats/min) or a step test (step height 40 cm for men, 33 cm for women, ascent rate - 22.5 cycles per minute) in for at least 5 minutes. Heart rate is recorded at the 5th minute of work. Calculation of MPK is carried out according to a special nomogram by I. Astrand (Fig. ) and the von Dobeln formula (Table. To calculate the MPK using the von Dobeln formula).
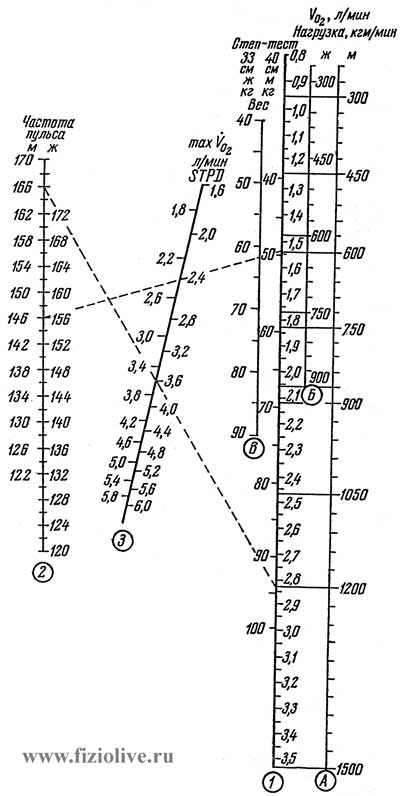
Astrand-Ryhming nomogram for determining BMD based on submaximal step test and bicycle ergometer test
K calculation of MPK (V O2max) using the von Dobeln formula
The MPF value found using the nomogram is corrected by multiplying by the “age factor” (Table ).
Age correction factors
Age-related correction factors to the values of maximum oxygen consumption according to the nomogram of I. Astrand (1960)
In table Determination of maximum oxygen consumption I. Astrand's nomogram is presented after calculation based on a submaximal load test on a bicycle ergometer.
Determination of maximum oxygen consumption*
| Men | ||||||||||
| Heart rate | Heart rate | Maximum oxygen consumption, l/min | ||||||||
| 300 kgm/min | 600 kgm/min | 900 kgm/min | 1200 kgm/min | 1500 kgm/min | 600 kgm/min | 900 kgm/min | 1200 kgm/min | 1500 kgm/min | ||
| 120 | 2,2 | 3,5 | 4,8 | - | - | 148 | 2,4 | 3,2 | 4,3 | 5,4 |
| 121 | 2,2 | 3,4 | 4,7 | - | - | 149 | 2,3 | 3,2 | 4,3 | 5,4 |
| 122 | 2,2 | 3,4 | 4,6 | - | - | 150 | 2,3 | 3,2 | 4,2 | 5,3 |
| 123 | 2,1 | 3,4 | 4,6 | - | - | 151 | 2,3 | 3,1 | 4,2 | 5,2 |
| 124 | 2,1 | 3,3 | 4,5 | 6,0 | - | 152 | 2,3 | 3,1 | 4,1 | 5,2 |
| 125 | 2,0 | 3,2 | 4,4 | 5,9 | - | 153 | 2,2 | 3,0 | 4,1 | 5,1 |
| 126 | 2,0 | 3,2 | 4,4 | 5,8 | - | 154 | 2,2 | 3,0 | 4,0 | 5,1 |
| 127 | 2,0 | 3,1 | 4,3 | 5,7 | - | 155 | 2,2 | 3,0 | 4,0 | 5,0 |
| 128 | 2,0 | 3,1 | 4,2 | 5,6 | - | 156 | 2,2 | 2,9 | 4,0 | 5,0 |
| 129 | 1,9 | 3,0 | 4,2 | 5,6 | - | 157 | 2,1 | 2,9 | 3,9 | 4,9 |
| 130 | 1,9 | 3,0 | 4,1 | 5,5 | - | 158 | 2,1 | 2,9 | 3,9 | 4,9 |
| 131 | 1,8 | 2,9 | 4,0 | 5,4 | - | 159 | 2,1 | 2,8 | 3,8 | 4,8 |
| 132 | 1,8 | 2,9 | 4,0 | 5,3 | - | 160 | 2,1 | 2,8 | 3,8 | 4,8 |
| 133 | 1,8 | 2,8 | 3,9 | 5,3 | - | 161 | 2,0 | 2,8 | 3,7 | 4,7 |
| 134 | 1,8 | 2,8 | 3,9 | 5,2 | - | 162 | 2,0 | 2,8 | 3,7 | 4,6 |
| 135 | 1,7 | 2,8 | 3,8 | 5,1 | - | 163 | 2,0 | 2,8 | 3,7 | 4,6 |
| 136 | 1,7 | 2,7 | 3,8 | 5,0 | - | 164 | 2,0 | 2,7 | 3,6 | 4,5 |
| 137 | 1,7 | 2,7 | 3,7 | 5,0 | - | 165 | 2,0 | 2,7 | 3,6 | 4,5 |
| 138 | 1,6 | 2,7 | 3,7 | 4,9 | - | 166 | 1,9 | 2,7 | 3,6 | 4,5 |
| 139 | 1,6 | 2,6 | 3,6 | 4,8 | - | 167 | 1,9 | 2,6 | 3,5 | 4,4 |
| 140 | 1,6 | 2,6 | 3,6 | 4,8 | 6,0 | 168 | 1,9 | 2,6 | 3,5 | 4,4 |
| 141 | - | 2,6 | 3,5 | 4,7 | 5,9 | 169 | 1,9 | 2,6 | 3,5 | 4,3 |
| 142 | - | 2,5 | 3,5 | 4,6 | 5,8 | 170 | 1,8 | 2,6 | 3,4 | 4,3 |
| 143 | - | 2,5 | 3,4 | 4,6 | 5,7 | - | - | - | - | - |
| 144 | - | 2,5 | 3,4 | 4,5 | 5,7 | - | - | - | - | - |
| 145 | - | 2,4 | 3,4 | 4,4 | 5,6 | - | - | - | - | - |
| 146 | - | 2,4 | 3,3 | 4,4 | 5,6 | - | - | - | - | - |
| 147 | - | 2,4 | 3,3 | 4,4 | 5,5 | - | - | - | - | - |
| Women | |||||||||||
| Heart rate | Maximum oxygen consumption, l/min | Heart rate | Maximum oxygen consumption, l/min | ||||||||
| 300 kgm/min | 450 kgm/min | 600 kgm/min | 750 kgm/min | 900 kgm/min | 300 kgm/min | 450 kgm/min | 600 kgm/min | 750 kgm/min | 900 kgm/min | ||
| 120 | 2,6 | 3,4 | 4,1 | 4,8 | - | 146 | 1,0 | 2,2 | 2,6 | 3,2 | 3,7 |
| 121 | 2,5 | 3,3 | 4,0 | 4,8 | - | 147 | 1,6 | 2,1 | 2,6 | 3,1 | 3,6 |
| 122 | 2,5 | 3,2 | 3,9 | 4,7 | - | 148 | 1,6 | 2,1 | 2,6 | 3,1 | 3,6 |
| 123 | 2,4 | 3,1 | 3,8 | 4,6 | - | 149 | - | 2,1 | 2,6 | 3,0 | 3,5 |
| 124 | 2,4 | 3,1 | 3,8 | 4,5 | - | 150 | - | 2,0 | 2,5 | 3,0 | 3,5 |
| 125 | 2,3 | 3,0 | 3,7 | 4,4 | - | 151 | - | 2,0 | 2,5 | 3,0 | 3,4 |
| 126 | 2,3 | 3,0 | 3,6 | 4,3 | - | 152 | - | 2,0 | 2,5 | 2,9 | 3,4 |
| 127 | 2,2 | 2,9 | 3,5 | 4,2 | - | 153 | - | 2,0 | 2,4 | 2,9 | 3,3 |
| 128 | 2,2 | 2,8 | 3,5 | 4,2 | 4,8 | 154 | - | 2,0 | 2,4 | 2,8 | 3,3 |
| 129 | 2,2 | 2,8 | 3,4 | 4,1 | 4,8 | 155 | - | 1,9 | 2,4 | 2,8 | 3,2 |
| 130 | 2,1 | 2,7 | 3,4 | 4,0 | 4,7 | 156 | - | 1,9 | 2,3 | 2,8 | 3,2 |
| 131 | 2,1 | 2,7 | 3,4 | 4,0 | 4,6 | 157 | - | 1,9 | 2,3 | 2,7 | 3,2 |
| 132 | 2,0 | 2,7 | 3,3 | 3,9 | 4,5 | 158 | - | 1,8 | 2,3 | 2,7 | 3,1 |
| 133 | 2,0 | 2,6 | 3,2 | 3,8 | 4,4 | 159 | - | 1,8 | 2,2 | 2,7 | 3,1 |
| 134 | 2,0 | 2,6 | 3,2 | 3,8 | 4,4 | 160 | - | 1,8 | 2,2 | 2,6 | 3,0 |
| 135 | 2,0 | 2,6 | 3,1 | 3,7 | 4,3 | 161 | - | 1,8 | 2,2 | 2,6 | 3,0 |
| 136 | 1,9 | 2,5 | 3,1 | 3,6 | 4,2 | 162 | - | 1,8 | 2,2 | 2,6 | 3,0 |
| 137 | 1,9 | 2,5 | 3,0 | 3,6 | 4,2 | 163 | - | 1,7 | 2,2 | 2,6 | 2,9 |
| 138 | 1,8 | 2,4 | 3,0 | 3,5 | 4,1 | 164 | - | 1,7 | 2,1 | 2,5 | 2,9 |
| 139 | 1,8 | 2,4 | 2,9 | 3,5 | 4,0 | 165 | - | 1,7 | 2,1 | 2,5 | 2,9 |
| 140 | 1,8 | 2,4 | 2,8 | 3,4 | 4,0 | 166 | - | 1,7 | 2,1 | 2,5 | 2,8 |
| 141 | 1,8 | 2,3 | 2,8 | 3,4 | 3,9 | 167 | - | 1,6 | 2,1 | 2,4 | 2,8 |
| 142 | 1,7 | 2,3 | 2,8 | 3,3 | 3,9 | 168 | - | 1,6 | 2,0 | 2,4 | 2,8 |
| 143 | 1,7 | 2,2 | 2,7 | 3,3 | 3,8 | 169 | - | 1,6 | 2,0 | 2,4 | 2,8 |
| 144 | 1,7 | 2,2 | 2,7 | 3,2 | 3,8 | 170 | - | 1,6 | 2,0 | 2,4 | 2,7 |
| 145 | 1,6 | 2,2 | 2,7 | 3,2 | 3,7 | - | - | - | - | - | - |
* Determination of maximum oxygen consumption by heart rate during exercise on a bicycle ergometer in men and women. These tables must be adjusted by age (see table. Age correction factors).
A special Gürtler nomogram has been developed for children and adolescents under 15 years of age.
Determination of MPK by direct method gives more accurate results. The subject performs a step-like increasing load on a bicycle ergometer or treadmill. The initial load power and subsequent “steps” are selected taking into account the gender, age and physical fitness of the subject. Direct determination of MPK is used when testing highly qualified athletes.
Depending on the sport and qualification, athletes start working with a power of 100 or 150 W, and female athletes - with 75 or 100 W. During the last 30 seconds of each “step” of the load, exhaled air is collected in a Douglas bag. Then a gas analysis is performed using a Holden apparatus or another device, and the amount of exhaled air is measured with a gas meter. There are automatic gas analyzers that allow you to continuously record the concentration of oxygen and carbon dioxide in the exhaled air flow during exercise. The electronic calculator of the latest models of analyzers automatically prints data on the level of oxygen consumption, pulmonary ventilation (minute volume of breathing), respiratory coefficient and other indicators on a paper tape every 20-30 seconds. The presence of devices of this type significantly increases the efficiency of testing athletes.
To compare the performance of individuals, it is not the absolute value of MPK (l/min) that is used, but a relative value. The latter is obtained by dividing MPK in ml/min by body weight in kilograms. The unit of relative indicator is ml/kg per 1 min.
In athletes, MPK is 3-5 l/min, in some cases - above 6 l/min. For cross-country skiers involved in rowing, road racing and other highly qualified athletes, the relative value of MPK reaches 80 l/kg per minute or more (Table Maximum oxygen consumption).
Maximum oxygen consumption*
| Kind of sport | Men | Women | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ski race |
83 | 63 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 80 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ice skating |
78 | 54 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Orientation Anaerobic performance is of great importance when performing extreme loads lasting from 30 s to 2 min. This type of work is typical for hockey players, middle-distance runners, speed skaters and representatives of other sports that train speed endurance. Among different indicators of anaerobic performance (maximum oxygen debt, maximum anaerobic power, etc.). The concentration of lactic acid (lactate) in arterial blood is most accessible for measurement. Lactate is determined during training and immediately after its completion. Blood is taken from a fingertip or earlobe. Lactic acid is determined by the Barker-Summerson method modified by Strom or by the enzymatic method. Normally, the concentration of lactic acid in the blood is 0.33-1.5 mmol/l. After physical activity, lactate ranges from 4-7 to 14-21 mmol/l. The indicators depend on the nature of the physical activity, age, gender and physical (functional) preparedness of the athlete. Under the influence of systematic intense physical activity, lactate decreases. Steps testThe step test is the most physiological, simple and accessible for physical fitness athletes. Usually a standard double step is used (each height is 23 cm). Other stepped ergometers are also used. Thus, V. Gottheiner (1968) adapts the height of the step to the length of the subject’s legs. With leg lengths up to 90 cm, the step height is 20 cm, with 90-99 cm - 30 cm, with 100-109 cm - 40 cm, and with 110 cm and above - 50 cm. In this case, the length of the subject’s leg is measured from the trochanteric point to the floor using the Gottheiner V. nomogram (Fig. ). The abscissa axis (AC) shows the leg length values, and the ordinate axis (AB) shows the step height values in centimeters. From the point of intersection of the perpendicular drawn from the point on the x-axis corresponding to the length of the leg of the subject with the line DE, draw a straight line to the ordinate axis and obtain a point corresponding to the desired height of the step. The rate of rise is controlled by a metronome. Each load stage lasts 4 minutes. Blood pressure and pulse are calculated before and after exercise.
Nomogram for determining the height of a step during a step test To determine the submaximal load level, you can use the table. Minimum number of ascents per step, which indicates the number of rises on a double step in 1 minute for 4 minutes, corresponding to 75% of the maximum oxygen consumption (MOC) for persons of average physical ability of different gender, weight and age. For an approximate assessment of the test results, use the table. Submaximal loads during step test. Above each column in parentheses is the heart rate (HR bpm), corresponding to the average physical ability of women and men of this age group. If the heart rate of the subject at the load specified for him differs by less than 10 beats/min from the value given in brackets, then his physical condition can be considered satisfactory. In the case when the heart rate is 10 or more below this value, the physical ability of the subject is above average, and if the heart rate is 10 or more beats/min above this value, then the physical ability is low. Submaximal loads during step test*
* Submaximal loads during the step test and their assessment for people of different ages, gender and body weight. The heart rate corresponding to the test results with the average physical ability of men and women of a given age group is indicated in parentheses (according to R. Shepard, 1969). W = BW x H x T x 1.33 where W is the load, (kgm/min), BW is body weight (kg), H is the height of the step (m), T is the number of ascents in 1 minute, 1.33 is a correction factor that takes into account the physical costs of descending the stairs, which account for 1/3 of the lifting costs. I. Ryhming (1953) proposed a step test, which can be used to determine BMD indirectly using a nomogram. The height of the steps for men is 40 cm, for women - 33 cm. The rate of ascent is 22 steps per minute, for 6 minutes. Then, according to the Astrand-Rieming nomogram (1954), MPK is determined (see Fig. ). Bicycle ergometryA bicycle ergometer is the most convenient device for conducting submaximal stress tests, as it provides the optimal opportunity to obtain accurate physiological data for assessing a person’s functional state and physical abilities. English | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

Determination of the level of physical performance in a person is carried out by using tests with maximum and submaximal levels of physical activity.
In tests with maximum power of physical activity, the test subject performs work with a progressive increase in its power until exhaustion (to failure). Such tests include the Nowacchi et al. test.
Tests with submaximal power loads are carried out by recording physiological indicators during work or after its completion. These include the well-known samples of S.P. Letunov, Harvard step test Master's test, etc. The fundamental feature of these tests is that there is an inversely proportional relationship between the power of muscular work and the duration of its execution, and in order to determine physical performance for such cases, special nomograms.
Testing physical performance based on heart rate has become widespread. This is explained by the fact that heart rate is an easily recorded physiological parameter. It is also important that heart rate is linearly related to the power of external mechanical work and the amount of oxygen consumed during exercise.
In sports, the PWC 170 test is used (PWC are the first letters of the English term “physical working capacity”), which is focused on achieving a certain heart rate (170 heart beats per minute). The subject is asked to perform bicycle ergometer or on a step test of two five-minute moderate-power loads with an interval of 3 minutes, after which the heart rate is measured. The PWC 170 indicator is calculated using the following formula:
PWC 170 = W 1 +(W 2 -W 1)∙ 170-f
where: W 1 and W 2 - power of the first and second loads;
f 1 and f 2 - heart rate at the end of the first and second load.
It is now generally accepted that a heart rate corresponding to 170 beats/min, from a physiological point of view, characterizes the beginning of the optimal working zone for the functioning of the cardiorespiratory system. From a methodological point of view, this is the beginning of a pronounced nonlinearity in the curve of the dependence of heart rate on the power of physical work. A significant physiological argument in favor of choosing the heart rate level in this test is the fact that at a pulse rate of more than 170 beats/min, an increase in minute blood volume, if it occurs, is already accompanied by a relative decrease in systolic blood volume.
The prospects for using this test in sports are very wide, since its principle is suitable for determining both the general and special performance of athletes.
Another common test is the Harvard Step Test. This test consists of climbing a step 50 cm high for men and 41 cm high for women for 5 minutes at a pace of 30 steps per minute (2 steps per second). After finishing work, within 30 seconds of the second minute of recovery, count the number of pulse beats and calculate the Harvard Step Test Index (HST) using the formula:
IGST = Operating time (s) 100
Number of pulse beats (s)
[(f 1 + f 2 + f 3) ∙ 2],
where t is the time to climb a step (s);
f 1, f 2, f 3 - the number of pulse beats in 30 s of the 2nd, 3rd and 4th minutes of recovery.
One of the most common and accurate methods is to determine physical performance by the value maximum oxygen consumption (MOC). This method is highly appreciated by the International Biological Program, which recommends using information on the value of aerobic productivity to assess physical performance.
As you know, the amount of oxygen consumed by muscles is equivalent to the work they do. Consequently, the body's oxygen consumption increases in proportion to the power of the work performed. MIC characterizes the maximum amount of oxygen that can be used by the body per unit of time.
MIC can be determined using maximum samples (direct method) and submaximal samples (indirect method). To determine MIC by the direct method, a bicycle ergometer or treadmill and gas analyzers are used. When using the direct method, the subject is required to desire to perform the work to failure, which is not always achievable. Several methods for indirectly determining MOC have been developed, based on the linear relationship between MOC and heart rate when working at a certain power. This dependence is expressed graphically on the corresponding nomograms and was described by a simple linear equation used for scientific and applied purposes for untrained individuals and athletes of speed-strength sports: MPC = 1.7 РWC 170 + 1240.
To determine MOC in highly qualified athletes of cyclic sports, V.L. Karpman (1987) proposes the following formula: MIC = 2.2 РWC 170 + 1070.
According to the author, both PWC 170 and MPC approximately equally characterize a person’s physical performance: the correlation coefficient between them is very high (0.7-0.9 according to different authors), although the relationship between these indicators is not strictly linear.
PWC 170 (for boxers) = 15.0 P + 300,
РWC 170 (for wrestlers) = 19.0 Р + 50, where
P - body weight.
It was found that athletes of the speed-strength group (wrestlers, boxers, gymnasts) lag behind even less qualified skiers, rowers, and football players in terms of PWC 170 and MPC.
Questions for self-control
1. What is human physical performance?
2. Name direct and indirect indicators of physical performance in sports.
3. Tell us about testing (working with maximum and submaximal power) in sports.
4. Describe the methods for determining physical performance in sports (PWC 170, step test, MPC).
5. List possible reserves for increasing physical performance in sports.
6. What is the purpose of testing in physical education and sports classes?
7. What should be understood by testing?
8. What loads are used for testing, and what conditions are necessary when performing them?
9. Are there differences in functional indicators between untrained and trained individuals under standard and extreme loads?
10. List the standard tests that are used to determine physical performance.
11. Give an example of specialized testing in your chosen sport.
12. Name the differences between an untrained and trained body during standard work.
13. By what indicators is the physical performance of athletes assessed when performing extreme loads?
14. What is meant by IPC and what does it characterize?
15. What functional systems does the IPC depend on?
16. In what tests is the MIC achieved?
17. Tell us about the direct method for determining MIC.
18. Tell us about the indirect method for determining MIC.
19. Name the optimal value of absolute and relative MOC that is achieved in skiers, swimmers and rowers.
20. Is there a relationship between heart rate, work power and VO2 max?
Laboratory work No. 6
Subject. Determination of physical performance using the PWC 170 test.
Target: master the methodology for conducting the PWC 170 test.
Object of study: Human.
Equipment: stopwatch, bicycle ergometer.
A bicycle ergometer (Greek ergon - work, metreo - I measure) is a device that is used to determine physical performance and exercise tolerance, as well as for training athletes, untrained, healthy and sick people.
Working on a bicycle ergometer is similar to riding a bicycle. The subject rotates the pedals with his feet, usually at a speed of 50-60 revolutions per minute. Changing the speed of rotation of the pedals or the braking force of the disc allows you to accurately dose the effort expended on the job. The operating power is expressed in watts. One watt is equal to 6 kg/m∙min.
Progress
1) determine the heart rate of the subjects at rest;
3) perform work with the first load power for 5 minutes;
5) take a three-minute rest between loads;
8) fill out a table reflecting the research results obtained;
9) plot the dependence of heart rate on the power of the load performed;
10) assess the physical performance of the subject (according to the table);
12) calculate relative indicators of physical performance among subjects;
13) make an analysis of the results obtained and conclusions.
Test procedure
The subject on a bicycle ergometer performs two loads of different power (W 1 and W 2) lasting 5 minutes each, with a 3-minute rest between them. Pedal speed - 60 rpm. The load is selected in such a way as to obtain several heart rate values in the range from 120 to 170 beats/min. At the end of each load (in the last minute), heart rate is measured (f 1 and f 2, respectively).
Graphs are constructed based on the data obtained. Load power indicators (W 1 and W 2) are plotted on the abscissa axis, and the corresponding heart rate indicators are plotted on the ordinate axis. At the intersection of perpendiculars, lowered to the corresponding points of the graph axes, coordinates 1 and 2 are found, a straight line is drawn through them until it intersects with the perpendicular restored from the heart rate point corresponding to 170 beats/min (coordinate 3). From it, a perpendicular is lowered onto the abscissa axis and the value of the load power is obtained at a heart rate equal to 170 beats/min.
Rice. 1. Graphical method for determining PWC 170:
f 1 and f 2 – heart rate at the first and second loads;
W 1 and W 2 – power of the first and second loads.
To simplify the calculation of the operating power during the two-stage test PWC 170, it can be determined using the formula: PWC 170 = W 1 +(W 2 -W 1)∙ 170-f,
where PWC 170 is the power of physical activity at a heart rate of 170 beats/min, W 1 and W 2 are the power of the first and second loads (kgm/min or W); f 1 and f 2 – heart rate in the last minute of the first and second loads (in 1 min).
Determining physical performance using the PWC 170 test gives reliable results if certain conditions are met:
1) loads must be performed without preliminary warm-up, otherwise test results will be underestimated;
2) correct choice of load power. The power of the second load should differ significantly from the first. The power of the second load should be determined depending on the type of sport and body weight, and the power of the second should be determined depending on the power of the first and heart rate after the first load.
The load (power) values can be selected from the tables (Table 14 and Table 15) and physical performance can be assessed (Table 16). An indicator that the load power has been chosen correctly can be the heart rate after completion. After the first load, the heart rate should be in the range of 100-120 beats/min, and after the second, as close as possible to 170 beats/min. The difference between the heart rate of the 1st and 2nd loads should be at least 40 beats/min.
If the conditions are met, the error in determining PWC 170 will be minimal.
Table 14
Power of the first load (kgm/min) according to Karpman V.L. (1988), recommended for determining PWC 170 in athletes
Table 15
Power of the second load (kgm/min) according to Karpman V.L. (1988) to determine PWC 170
Related information.
When assessing performance in restoring heart rate, two patterns of the body’s response to standard loads are taken into account as the main criteria:
a) economy of the reaction and
b) fast recovery.
1. roufier sample. Control heart rate calculations are performed in the supine position before, after exercise and at the end of the 1st minute of recovery for 15 seconds (P1, P2, P3). As a load – 30 squats in 45 seconds.
Ruffier index (IR) = (4*(Р1+Р2+р3)) / 10.
Performance is assessed qualitatively (high, good, average, good, bad).
2. Harvard step test.
The test consists of climbing a step of a certain height, depending on age and gender, for a strictly defined time - 5 minutes. The number of steps per step is 30 times per minute with a metronome rhythm of 120 beats. / min. To calculate the classic IHST, the pulse is calculated during the first 30 seconds of the second (P1), third (P2) and fourth (P3) minutes of recovery.
IGST = T*100 / ((P1+P2+P3)*2)
Assessment of physical performance according to IGST: less than 55 – weak; 55-64 below average; 65-79 – average; 80-89 – good; more than 90 – excellent.
3. Querg test.
The test consists of four exercises, following each other without interruption:
30 squats in 30 seconds;
Running at maximum speed – 30 seconds;
Running in place at a frequency of 150 steps/min. - 3 minutes;
jumping rope – 1 min.
The pulse is counted for 30 seconds immediately after the test (P1), after 2 minutes (P2) and after 4 minutes (P3) of recovery.
Querg Index (IC) = 15000 / (P1+P2+P3).
This test can be used as a mass experiment.
MAXIMUM OXYGEN CONSUMPTION.
To more accurately determine the level of physical condition, it is customary to evaluate it in relation to proper MPC (DMPC) values, corresponding to the average normal values for a given age and gender. They can be calculated using the following formulas:
for men:DMPK== 52-(0.25X age), (1)
for women: DMPC == 44- (0.20X age). (2)
Knowing the proper value of MIC for a given individual and its actual value, it is possible to determine %DMK:
%DMPK==MPK / DMPK*100% (3)
Definition actual MPC value the direct method is quite difficult, so in mass physical culture they have become widespread indirect methods determining maximum aerobic performance by calculation.
1.The most informative istestP.W.C. 170 -- physical performance at a pulse of 170 beats/min. The subject is offered two relatively small loads on a bicycle ergometer or step (5 minutes each, with a rest interval of 3 minutes). At the end of each load (once a steady state is reached), the heart rate is calculated. The calculation is made using the formula:
P.W.C. 170 ==N1+(N2 - N1)*(170-f1/f2-f1) (4)
– where N1 is the power of the first load; N2power of the second load (W converted to kgm/min); f1 - heart rate at the end of the first load; f2 - heart rate at the end of the second load. When using a step N1.2 = 1.5*P*h* n, where P – weight (kg), h – step height (m), n – walking frequency (times/min). The calculated MIC value (l/min) is determined according to the formula of V. L. Karpman for people with a low level of fitness:
MPC=1.7.*PWC 170 +1240 (5).
MPC=2.2.*PWC 170 +1070 (for athletes).
In children PWC 170 determined in a modified single 5-minute test according to I.A. Kornienko (1978):
P.W.C. 170 = N*(170 – state of emergency) / (ChN – state of emergency),
Where N – load power, HR – heart rate at rest (min), HR – heart rate after exercise (min).
MIC calculationaccording to Dobeln's formula requires performing a single load of submaximal power on a bicycle ergometer or in a step test:MIC = 1.29* root of N/f-60*Twhere T is the age coefficient; f--heart rate at the 5th minute of work; N -- load power.
2. In addition, the IPC can be determined in Astranda-Riming testaccording to nomogram. The subject performs a single load of submaximal power on a bicycle ergometer for 5 minutes (heart rate approximately 75 % from maximum) or in the Step test (climbing a step 40 cm high for men and 33 cm high for women at a pace of 22.5 steps per minute). At the end of the load, the heart rate is determined. The calculation is carried out according to the Astrand - Rimming nomogram.Knowing the power of the work performed and the heart rate, the estimated level of MOC can be determined using the nomogram. To take into account the age of the subject, the resulting value must be multiplied by an age correction factor.
3. During a mass examination of individuals engaged in recreational physical culture, the value of MIC and the level of physical condition can be determined using 1 .5 mile Cooper test under natural training conditions. To perform this test you must run a distance of 2400 m at the highest possible speed (6 laps along a 400-meter stadium track). When comparing the test results with the data obtained when determining PWC170 on a bicycle ergometer (B. G. Milner, 1985), a high degree of correlation between them was revealed, which made it possible to calculate a linear regression equation:
PWC170=(33.6-1.3Tk)+-1.96
where Tk is the Cooper test in fractions of a minute (for example, the test result of 12 min 30 s is 12.5 min), and PWC170 is measured in kgm/min/kg. Knowing the PWC170 test value, according to formula (5) MPC=1.7.*PWC170+1240, you can calculate the MIC and determine the level of physical condition of the subject.
Physical performance is an integral indicator of the functional state of the body. Assessment of the level of physical condition can be made not only by the value of MIC, but also directly by direct indicators of physical performance.
These include PWC170 test And submaximal bicycle ergometer test. These indicators are measured in units of power of the work performed (kgm/min or W). With age, the functionality of the circulatory system decreases, so the power of work is determined by:
for people 40 years old - at heart rate 150 beats/min PWC170,
50 years - 140 beats/min,
60 years old - 130 beats/min.
Average normalabsolute The PWC170 test indicators consider the load power:
in young men1000 kgm/min,
for women - 700 kgm/min.
More informative are not absolute ones, but relative s Test values - work power per 1 kg of body weight:
for young men the average norm is 15.5 kgm/min/kg,
for women -- 10.5 kgm/min/kg.

