Cardiac surgeon
Higher education:
Cardiac surgeon
Kabardino-Balkarian State University them. HM. Berbekova, Faculty of Medicine (KBSU)
Level of education - Specialist
Additional education:
Certification cycle for the Clinical Cardiology program
Moscow medical Academy them. THEM. Sechenov
Not all people without medical education are aware of congenital heart defects. This pathology is often detected in childhood and is difficult to treat. Drug therapy in this situation is ineffective. Many children with this pathology become disabled.
Heart defects from birth
The classification of congenital defects is known to every experienced cardiologist. This is a large group of diseases that affect various structures of the heart and blood vessels. The prevalence of this congenital pathology among children is about 1%. Some vices are incompatible with life.
In cardiology it is often various diseases are combined with each other. Congenital and acquired heart defects worsen a person’s quality of life. The following types of defects are distinguished:
- accompanied by increased blood flow in the lungs;
- with normal blood flow in the pulmonary circle;
- with reduced blood supply to the lung tissue;
- combined.

There is a classification based on the presence of cyanosis. It includes congenital heart defects of the “blue” and “white” types. The most frequently diagnosed diseases are:
- open duct of Botallus;
- coarctation of the aorta;
- tetralogy of Fallot;
- valvular atresia;
- defect of the interventricular and interatrial septa;
- narrowing of the aortic lumen;
- pulmonary artery stenosis.
Main etiological factors
For congenital heart defects, the causes vary. Highest value have the following etiological factors:
- chromosomal disorders;
- gene mutations;
- transferred viral infections mothers while carrying a baby;
- infection of a child with the rubella virus;
- alcohol syndrome;
- exposure to chemicals (heavy metals, pesticides, alcohol);
- irradiation;
- inhalation of polluted air;
- drinking poor quality water;
- harmful occupational factors;
- taking toxic medications during pregnancy.
The causes of heart defects often lie in external factors. Diseases such as chickenpox, herpes, hepatitis, toxoplasmosis, rubella, syphilis, tuberculosis, and HIV infection are dangerous for the unborn baby. Narcotic drugs (amphetamines) have a teratogenic effect.

Maternal smoking has an adverse effect on the development of the fetus. Congenital defects development is more often diagnosed in those children who were born to mothers with diabetes mellitus. Risk factors are:
- smoking;
- alcohol addiction;
- advanced age of father and mother;
- taking antibiotics in the 1st and 3rd trimesters;
- history of toxicosis;
- taking hormonal drugs.
The most frequently detected pathologies are patent ductus arteriosus and VSD.
Opening of the ductus arteriosus
During intrauterine development, the child’s cardiovascular system has its own characteristics. An example is patent ductus arteriosus. This is an anastomosis connecting the pulmonary artery and the aorta. Normally, this duct closes within 2 months after birth. This does not happen if the child’s development is impaired. Patent ductus arteriosus (PDA) persists.
Each doctor has a presentation on congenital heart defects. It should indicate that this pathology occurs quite often. In boys, PDA is diagnosed less frequently. Its share in the overall structure of congenital anomalies is about 10%. The disease is combined with another pathology - coarctation of the aorta, vasoconstriction or tetralogy of Fallot.
This heart disease is more often found in premature babies. After childbirth, it leads to a delay in physical development. In children weighing less than 1 kg, patent ductus arteriosus (PDA) is diagnosed in 80% of cases. Risk factors are:
- asphyxia during childbirth;
- burdened heredity;
- parents living in the highlands;
- carrying out oxygen therapy.
This disease belongs to the “pale” type of defects. This pathology has its own code in ICD-10. PDA is characterized by the discharge of oxygen-rich blood from the aorta into the pulmonary artery. This causes hypertension, which increases the load on the heart. This is how hypertrophy and dilatation of the left sections develop.
Patent ductus arteriosus (PDA) occurs in 3 stages. The most dangerous is grade 1. It can lead to death. Stage 2 is observed between the ages of 2 and 20 years. At this stage, overload of the right ventricle of the heart and an increase in the volume of blood volume in the pulmonary circulation system are detected. At stage 3, sclerotic changes develop in the lungs.

You need to know not only the causes of congenital heart defects, but also their symptoms. With an open duct, the following symptoms are possible:
- pale or cyanotic skin;
- disturbance of sucking;
- scream;
- straining;
- poor weight gain;
- developmental delay;
- frequent respiratory diseases;
- shortness of breath on exertion;
- violation heart rate.
Complications include development vascular insufficiency and inflammation of the endocardium. Many patients have no symptoms.
With congenital heart disease, the bicuspid and aortic valves can also be affected. This is a dangerous pathology that requires surgery. The aortic valve is located between the left ventricle and the aorta. Its flap closes, blocking the path for the return flow of blood. With a vice, this process is disrupted. Some of the blood rushes back into the left ventricle.
Its overflow causes stagnation of blood in the small circle. Nice presentation on this topic states that the basis of hemodynamic disorders are the following changes:
- congenital deficiency of one valve;
- valve sagging;
- different sizes of sashes;
- underdevelopment;
- the presence of a pathological hole.

This cardiac defect can be either congenital or acquired. In the first case, most often the violations are minor, but if the person is not treated, complications are possible. With this congenital heart defect, symptoms include chest pain, palpitations, swelling of the extremities, shortness of breath, tinnitus, occasional fainting, and dizziness.
Brain function is impaired. Objective signs of aortic valve insufficiency are:
- pale skin;
- pulsation of the carotid arteries;
- constriction of the pupils;
- protrusion of the chest;
- enlargement of the boundaries of the heart;
- pathological heart murmurs;
- heart rate acceleration;
- increase in pulse pressure.
All these symptoms appear if 20-30% of the blood returns back to the ventricle. Congenital malformations can appear in early childhood or after 10-20 years, when the heart cannot compensate for hemodynamic disturbances.
Aortic stenosis and atresia
In the group of congenital heart defects, the classification distinguishes coarctation of the aorta. This vessel is the largest. It has ascending and descending parts, as well as an arc. In the group of congenital heart diseases, coarctation of the aorta is common. With this pathology, a narrowing of the lumen or atresia (overgrowth) of the vessel is observed. The aortic isthmus is involved in the process.
This anomaly occurs in children. The share of this defect in the overall structure of cardiac pediatric pathology is about 7%. Most often, narrowing is observed in the area of the terminal part of the aortic arch. The stenosis is shaped like an hourglass. The length of the narrowed area often reaches 5-10 cm. This pathology often leads to atherosclerosis.
Coarctation causes left ventricular hypertrophy, increased stroke volume and dilation of the ascending aorta. Collaterals (bypass network of vessels) are formed. Over time, they become thinner, which leads to the formation of aneurysms. Possible brain damage. You need to know not only what coarctation of the aorta is, but also how it manifests itself.

With this defect, the following clinical signs are revealed:
- weight gain;
- growth retardation;
- dyspnea;
- signs of pulmonary edema;
- decreased vision;
- headache;
- dizziness;
- hemoptysis;
- nosebleeds;
- convulsions;
- abdominal pain.
Clinical picture determined by the period of development of coarctation. In the decompensation stage, severe heart failure develops. The percentage of deaths is high. Most often this is observed between the ages of 20-40 years. When brain function is impaired, neurological symptoms are pronounced. This includes chilliness of the extremities, headache, fainting, convulsions, and lameness.
Tetralogy and triad of Fallot
Congenital heart defects in adults and children include Fallot's triad. This is a combined defect that includes:
- defect of the septum between the atria;
- narrowing of the pulmonary artery;
- right ventricular hypertrophy.
The reason is a violation of embryogenesis in the 1st trimester of pregnancy. It is during this period that the heart is formed. Symptoms are caused primarily by narrowing of the pulmonary artery. This is a large vessel extending from the right ventricle of the heart. It's paired. They begin the large circle of blood circulation.
With severe stenosis, overload of the right ventricle occurs. The pressure in the cavity of the right atrium increases. The following violations occur:
- tricuspid valve insufficiency;
- decrease in minute blood volume in the pulmonary circle;
- increase in minute volume in a large circle;
- decrease in blood oxygen saturation.

Like other congenital malformations, Fallot's triad early age leaks hidden. A common symptom is fatigue. Along with the triad, tetralogy of Fallot often develops. It includes pulmonary stenosis, changes in the position of the aorta (dextroposition), right ventricular hypertrophy and VSD.
Tetralogy of Fallot belongs to the group of cyanotic (“blue”) defects. Its share is 7-10%. This pathology is named after the French doctor. This disease develops at 1-2 months of intrauterine development. Tetralogy of Fallot is often associated with anomalies ears, oligophrenia, vices internal organs, dwarfism.
In the early stages, symptoms are nonspecific. Later, tetralogy of Fallot leads to dysfunction of the brain and other vital important organs. The development of hypoxic coma and paresis is possible. Young children often suffer from infectious diseases. The main manifestation of the defect is cyanotic attacks accompanied by shortness of breath.
Patient examination plan
Treatment of congenital heart defects is carried out after excluding other (acquired) diseases. Any quality presentation states that the following studies are required to identify the disease:
- listening to the heart;
- percussion;
- electrocardiography;
- X-ray examination;
- registration of sound signals;
- Holter monitoring;
- coronary angiography;
- probing of cavities.

The diagnosis of congenital heart disease is made based on the results of instrumental studies. With congenital anomalies, the changes are very different. Tetralogy of Fallot shows the following symptoms:
- symptom " drumsticks" and "watch glasses";
- heart hump;
- rough noise in the 2-3 intercostal space to the left of the sternum;
- weakening of 2 tones in the pulmonary artery area;
- deviation of the electrical axis of the heart to the right;
- expansion of the boundaries of the organ;
- increased pressure in the right ventricle.
The main diagnostic criteria for patent ductus arteriosus are an increase in the boundaries of the myocardium, a change in its shape, simultaneous filling of the aorta and pulmonary artery with contrast, and manifestations of hypertension. If congenital malformations are suspected, brain function must be assessed. Studies such as computed tomography and magnetic resonance imaging are more informative. The valves (bicuspid, tricuspid, aortic and pulmonary) are assessed.
Therapeutic tactics for congenital defects
If there are “blue” or “white” heart defects, then radical or conservative treatment. If a patent ductus arteriosus is detected in a premature baby, it is necessary to use prostaglandin synthesis inhibitors. This allows you to speed up the healing of the anastomosis. If such therapy does not have an effect, then after 3 weeks of birth, surgery can be performed.
It can be open or endovascular. The prognosis for congenital and acquired heart defects is determined by the severity of hemodynamic disorders. When a person is diagnosed with tetralogy of Fallot, only surgical treatment is effective. All patients are hospitalized. When cyanotic attacks develop, the following are used:
- oxygen therapy;
- administration of infusion solutions;
- Eufillin.
In severe cases, an anastomosis is performed. Often organized palliative operations. Bypass surgery is performed. The most radical and effective measure is to perform plasty of the ventricular septal defect. The patency of the pulmonary artery is necessarily restored.
If congenital coarctation of the aorta is detected, surgery should be performed early. In case of development of a critical defect, surgical treatment is indicated in the child under 1 year of age. In case of irreversible pulmonary hypertension, surgery is not performed. The most commonly used types of surgical interventions are:
- plastic reconstruction of the aorta;
- resection followed by prosthetics;
- formation of bypass anastomoses.
Thus, congenital heart abnormalities can appear both in childhood and later. Some diseases require radical treatment.
From this article you will learn: what types of heart diseases are there (congenital and acquired). Their causes, symptoms and treatment methods (medical and surgical).
Article publication date: 03/02/2017
Article updated date: 05/29/2019
Cardiovascular diseases are one of the leading causes of death. Russian statistics show that about 55% of all deceased citizens suffered from diseases of this group.
Therefore, knowing the signs of cardiac pathologies is important for everyone in order to identify the disease in time and begin treatment immediately.
It is equally important to undergo a preventive examination by a cardiologist at least once every 2 years, and from the age of 60 - every year.
The list of heart diseases is extensive, it is presented in the content. They are much easier to treat if diagnosed at an early stage. Some of them are completely curable, others are not, but in any case, if you start therapy at early stage, can be avoided further development pathologies, complications and reduce the risk of death.
Coronary heart disease (CHD)
This is a pathology in which there is insufficient blood supply to the myocardium. The cause is atherosclerosis or thrombosis of the coronary arteries.

Classification of IHD
Acute coronary syndrome is worth talking about separately. Its symptom is a prolonged (more than 15 minutes) attack of chest pain. This term does not denote a separate disease, but is used when it is impossible to distinguish myocardial infarction from myocardial infarction based on symptoms and ECG. The patient is given a preliminary diagnosis of “acute coronary syndrome” and immediately begins thrombolytic therapy, which is needed for any acute form of coronary artery disease. The final diagnosis is made after blood tests for markers of infarction: cardiac troponin T and cardiac troponin 1. If their levels are elevated, the patient has had myocardial necrosis.
Symptoms of IHD
A sign of angina pectoris is attacks of burning, squeezing pain behind the sternum. Sometimes the pain radiates to the left side, to various parts of the body: shoulder blade, shoulder, arm, neck, jaw. Less often, pain is localized in the epigastrium, so patients may think that they have problems with the stomach and not with the heart.
With stable angina, attacks are provoked by physical activity. Depending on the functional class of angina (hereinafter referred to as FC), pain can be caused by stress of varying intensity.
| 1 FC | The patient tolerates daily activities well, such as long walking, light jogging, climbing stairs, etc. Attacks of pain occur only during high-intensity physical activity: fast running, repeated weight lifting, playing sports, etc. |
|---|---|
| 2 FC | An attack may occur after walking more than 0.5 km (7–8 minutes without stopping) or climbing stairs higher than 2 floors. |
| 3 FC | A person’s physical activity is significantly limited: walking 100–500 m or climbing to the 2nd floor can trigger an attack. |
| 4 FC | Seizures are provoked by even the slightest physical activity: walking less than 100 m (for example, moving around the house). |

Unstable angina differs from stable angina in that attacks become more frequent, begin to appear at rest, and can last longer - 10-30 minutes.
Cardiosclerosis is manifested by chest pain, shortness of breath, fatigue, swelling, and rhythm disturbances.
According to statistics, about 30% of patients die from this heart disease within 24 hours without seeing a doctor. Therefore, carefully study all the signs of MI in order to call an ambulance in time.
Symptoms of MI
| Form | Signs |
|---|---|
| Anginal – the most typical | Pressing, burning pain in the chest, sometimes radiating to left shoulder, arm, shoulder blade, left side of the face. The pain lasts from 15 minutes (sometimes even a day). Not removable by Nitroglycerin. Analgesics only weaken it temporarily. Other symptoms: shortness of breath, arrhythmias. |
| Asthmatic | An attack of cardiac asthma develops, caused by acute failure of the left ventricle. Main signs: feeling of suffocation, lack of air, panic. Additional: cyanosis of the mucous membranes and skin, accelerated heartbeat. |
| Arrhythmic | High heart rate, low blood pressure, dizziness, possible fainting. |
| Abdominal | Pain in the upper abdomen that radiates to the shoulder blades, nausea, vomiting. Often even doctors initially confuse it with gastrointestinal diseases. |
| Cerebrovascular | Dizziness or fainting, vomiting, numbness in an arm or leg. The clinical picture of such an MI is similar to an ischemic stroke. |
| Asymptomatic | The intensity and duration of pain is the same as with normal pain. There may be slight shortness of breath. Distinctive feature pain - Nitroglycerin tablet does not help. |

Treatment of coronary artery disease
| Stable angina | Relieving an attack - Nitroglycerin. Long-term therapy: Aspirin, beta-blockers, statins, ACE inhibitors. |
|---|---|
| Unstable angina | Emergency care: call an ambulance if an attack of greater intensity than usual occurs, and also give the patient an Aspirin tablet and a Nitroglycerin tablet every 5 minutes 3 times. In the hospital, the patient will be given calcium antagonists (Verapamil, Diltiazem) and Aspirin. The latter will need to be taken on an ongoing basis. |
| Myocardial infarction | Emergency help: call a doctor immediately, 2 tablets of Aspirin, Nitroglycerin under the tongue (up to 3 tablets with an interval of 5 minutes). Upon arrival, doctors will immediately begin this treatment: they will inhale oxygen, administer a morphine solution, if Nitroglycerin does not relieve the pain, and administer Heparin to thin the blood. Further treatment: pain relief with intravenous administration Nitroglycerin or narcotic analgesics; preventing further necrosis of myocardial tissue with the help of thrombolytics, nitrates and beta-blockers; constant use of Aspirin. Restore blood circulation in the heart with the help of such surgical operations: coronary angioplasty, stenting, . |
| Cardiosclerosis | The patient is prescribed nitrates, cardiac glycosides, ACE inhibitors or beta-blockers, Aspirin, diuretics. |

Chronic heart failure
This is a condition of the heart in which it is unable to fully pump blood throughout the body. The reason is heart and vascular diseases (congenital or acquired defects, ischemic heart disease, inflammation, atherosclerosis, hypertension, etc.).

In Russia, more than 5 million people suffer from CHF.
Stages of CHF and their symptoms:
- 1 – initial. This is mild left ventricular failure that does not lead to hemodynamic (circulatory) disturbances. There are no symptoms.
- Stage 2A. Poor circulation in one of the circles (usually the small circle), enlargement of the left ventricle. Signs: shortness of breath and palpitations with little physical exertion, cyanosis of the mucous membranes, dry cough, swelling of the legs.
- Stage 2B. Hemodynamics are impaired in both circles. The chambers of the heart undergo hypertrophy or dilatation. Signs: shortness of breath at rest, aching pain in the chest, blue tint of the mucous membranes and skin, arrhythmias, cough, cardiac asthma, swelling of the limbs, abdomen, enlarged liver.
- Stage 3. Severe circulatory disorders. Irreversible changes in the heart, lungs, blood vessels, kidneys. All the signs characteristic of stage 2B intensify, and symptoms of damage to internal organs appear. Treatment is no longer effective.

Treatment
First of all, treatment of the underlying disease is necessary.
Symptomatic drug treatment is also carried out. The patient is prescribed:
- ACE inhibitors, beta blockers or aldosterone antagonists - to lower blood pressure and prevent further progression of heart disease.
- Diuretics - to eliminate edema.
- Cardiac glycosides - for the treatment of arrhythmias and improvement of myocardial performance.
Valve defects
There are two typical types of valve pathologies: stenosis and insufficiency. With stenosis, the valve lumen is narrowed, making it difficult to pump blood. In case of insufficiency, the valve, on the contrary, does not close completely, which leads to the outflow of blood in the opposite direction.

More often, such heart valve defects are acquired. Appear in the background chronic diseases(for example, coronary artery disease), previous inflammation or poor lifestyle.
The aortic and mitral valves are most susceptible to disease.
Symptoms and treatment of the most common valve diseases:
| Name | Symptoms | Treatment |
|---|---|---|
| Aortic stenosis | At the initial stage there are no symptoms, so it is very important to regularly undergo preventive heart examinations. At a severe stage, attacks of angina pectoris, fainting during physical exertion, pale skin, and low systolic blood pressure appear. |
Drug treatment of symptoms (due to valve defects). Valve replacement. |
| Aortic valve insufficiency | Increased heart rate, shortness of breath, cardiac asthma (attacks of suffocation), fainting, low diastolic blood pressure. | |
| Mitral stenosis | Shortness of breath, enlarged liver, swelling of the abdomen and limbs, sometimes hoarseness of the voice, rarely (in 10% of cases) pain in the heart. | |
| Mitral valve insufficiency | Shortness of breath, dry cough, cardiac asthma, swelling of the legs, pain in the right hypochondrium, aching pain in the heart. |
Mitral valve prolapse

Another common pathology is. Occurs in 2.4% of the population. This is a congenital defect in which the valve leaflets “sink” into the left atrium. In 30% of cases it is asymptomatic. In the remaining 70% of patients, doctors note shortness of breath, pain in the heart area, accompanied by nausea and a feeling of a “lump” in the throat, arrhythmias, fatigue, dizziness, and frequent increases in temperature to 37.2–37.4.
Treatment may not be required if the disease is asymptomatic. If the defect is accompanied by arrhythmias or pain in the heart, prescribe symptomatic therapy. If the valve changes significantly, surgical correction is possible. Since the disease progresses with age, patients need to be examined by a cardiologist 1-2 times a year.
Ebstein's anomaly

Ebstein's anomaly is a displacement of the tricuspid valve leaflets into the right ventricle. Symptoms: shortness of breath, paroxysmal tachycardia, fainting, swelling of the veins in the neck, enlargement of the right atrium and the upper part of the right ventricle.
Treatment for asymptomatic cases is not carried out. If the symptoms are severe, surgical correction or valve transplantation is performed.
Congenital heart defects
TO congenital anomalies structures of the heart include:
- Atrial septal defect is the presence of communication between the right and left atria.
- A ventricular septal defect is an abnormal communication between the right and left ventricles.
- The Eisenmenger complex is a high-lying ventricular septal defect, the aorta is displaced to the right and connects simultaneously with both ventricles (aortic dextroposition).
- Patent ductus arteriosus - the communication between the aorta and the pulmonary artery, which is normally present at the embryonic stage of development, is not closed.
- Tetralogy of Fallot is a combination of four defects: ventricular septal defect, aortic dextroposition, pulmonary stenosis and right ventricular hypertrophy.

Congenital heart defects - signs and treatment:
| Name | Symptoms | Treatment |
|---|---|---|
| Atrial septal defect | At small defect signs begin to appear in middle age: after 40 years. This is shortness of breath, weakness, fatigue. Over time, chronic heart failure develops with all the characteristic symptoms. How larger sizes defect, the sooner symptoms begin to appear. | Surgical closure of the defect. Doesn't always happen. Indications: ineffective drug treatment CHF, retardation in physical development in children and adolescents, increased blood pressure in the pulmonary circle, arteriovenous discharge. Contraindications: venoarterial shunt, severe left ventricular failure. |
| Ventricular septal defect | If the defect is less than 1 cm in diameter (or less than half the diameter of the aortic orifice), only shortness of breath is characteristic during physical activity of moderate intensity. If the defect is larger than the specified size: shortness of breath with light exertion or at rest, heart pain, cough. |
Surgical closure of the defect. |
| Eisenmenger complex | Clinical picture: bluish skin, shortness of breath, hemoptysis, signs of CHF. | Medication: beta-blockers, endothelin antagonists. Surgery to close the septal defect, correct the aortic origin, and replace the aortic valve is possible, but patients often die during the procedure. The average life expectancy of a patient is 30 years. |
| Tetralogy of Fallot | Blue tint of mucous membranes and skin, retarded growth and development (both physical and intellectual), seizures, low blood pressure, symptoms of heart failure. Average life expectancy is 12–15 years. 50% of patients die before the age of 3 years. |
Surgical treatment is indicated for all patients without exception. In early childhood, surgery is performed to create an anastomosis between the subclavian and pulmonary arteries to improve blood circulation in the lungs. At 3–7 years of age, radical surgery can be performed: simultaneous correction of all 4 anomalies. |
| Patent ductus arteriosus | A long time passes without clinical signs. Over time, shortness of breath and palpitations, pallor or a blue tint to the skin, and low diastolic blood pressure appear. | Surgical closure of the defect. Indicated for all patients, except for those who have right-to-left shunting. |
Inflammatory diseases
Classification:
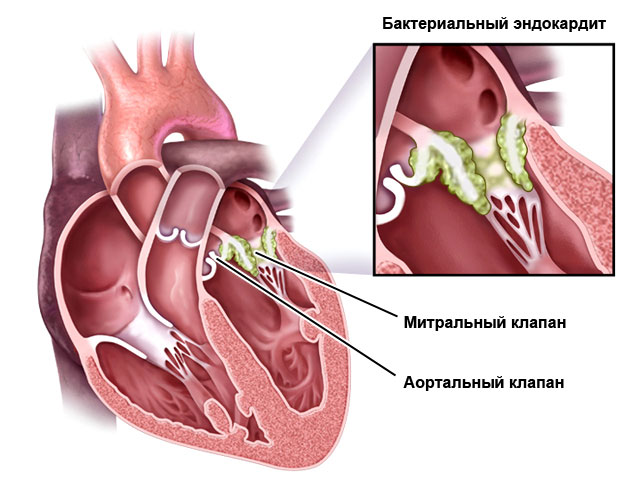
- Endocarditis – affects the inner lining of the heart, the valves.
- Myocarditis – muscle membrane.
- Pericarditis - the pericardial sac.
They can be caused by microorganisms (bacteria, viruses, fungi), autoimmune processes (for example, rheumatism) or toxic substances.
Heart inflammation can also be complications of other diseases:
- tuberculosis (endocarditis, pericarditis);
- syphilis (endocarditis);
- flu, sore throat (myocarditis).
Pay attention to this and consult a doctor promptly if you suspect flu or sore throat.
Symptoms and treatment of inflammation
| Name | Symptoms | Treatment |
|---|---|---|
| Endocarditis | High temperature (38.5–39.5), increased sweating, rapidly developing valve defects (detected by echocardiography), heart murmurs, enlarged liver and spleen, increased fragility of blood vessels (hemorrhages under the nails and in the eyes can be seen), thickening of the fingertips. | Antibacterial therapy for 4–6 weeks, valve transplantation. |
| Myocarditis | It can occur in several ways: attacks of pain in the heart; symptoms of heart failure; or with extrasystole and supraventricular arrhythmias. An accurate diagnosis can be made based on a blood test for cardiac-specific enzymes, troponins, and leukocytes. | Bed rest, diet (No. 10 with salt restriction), antibacterial and anti-inflammatory therapy, symptomatic treatment of heart failure or arrhythmias. |
| Pericarditis | Chest pain, shortness of breath, palpitations, weakness, cough without sputum, heaviness in the right hypochondrium. | Non-steroidal anti-inflammatory drugs, antibiotics, in severe cases - subtotal or total pericardiectomy (removal of part or all of the pericardial sac). |
Rhythm disorders
Reasons: neuroses, obesity, unhealthy diet, cervical osteochondrosis, bad habits, intoxication with drugs, alcohol or narcotic substances, IHD, cardiomyopathies, heart failure, ventricular premature excitation syndromes. The latter are heart diseases in which there are additional impulse pathways between the atria and ventricles. You will read about these anomalies in a separate table.
Characteristics of rhythm disturbances:
| Name | Description |
|---|---|
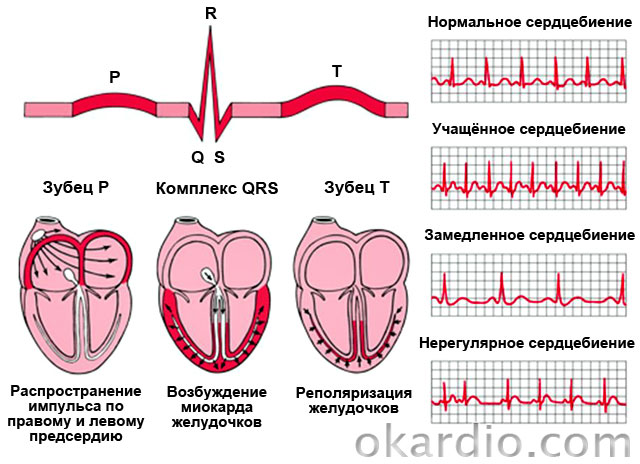
| Sinus tachycardia | Rapid heartbeat (90–180 per minute) while maintaining the normal rhythm and normal pattern of impulse propagation throughout the heart. |
| Atrial fibrillation (flicker) | Uncontrolled, irregular and frequent (200–700 per minute) atrial contractions. |
| Atrial flutter | Rhythmic contractions of the atria with a frequency of about 300 per minute. |
| Ventricular fibrillation | Chaotic, frequent (200–300 per minute) and incomplete ventricular contractions. The absence of a complete reduction provokes acute failure blood circulation and fainting. |
| Ventricular flutter | Rhythmic contractions of the ventricles with a frequency of 120–240 per minute. |
| Paroxysmal supraventricular (supraventricular) tachycardia | Attacks of rhythmic rapid heartbeat (100–250 per minute) |
| Extrasystole | Spontaneous contractions out of rhythm. |
| Conduction disorders (sinoatrial block, interatrial block, atrioventricular block, bundle branch block) | Slowing down the rhythm of the entire heart or individual chambers. |
Syndromes of premature excitation of the ventricles:
| WPW syndrome (Wolf–Parkinson–White syndrome) | CLC syndrome (Clerc-Levy-Christesco) |
|---|---|
| Signs: paroxysmal (paroxysmal) supraventricular or ventricular tachycardia (in 67% of patients). Accompanied by a feeling of increased heartbeat, dizziness, and sometimes fainting. | Symptoms: tendency to attacks of supraventricular tachycardia. During them, the patient feels a strong heartbeat and may feel dizzy. |
| Cause: the presence of a bundle of Kent, an abnormal pathway between the atrium and ventricle. | Cause: the presence of a James bundle between the atrium and the atrioventricular junction. |
| Both diseases are congenital and quite rare. | |
Treatment of rhythm disturbances
It consists of treating the underlying disease, adjusting diet and lifestyle. Also prescribed antiarrhythmic drugs. Radical treatment for severe arrhythmias - installation of a defibrillator-cardioverter, which will “set” the rhythm of the heart and prevent ventricular or atrial fibrillation. In case of conduction disturbances, electrical cardiac stimulation is possible.

Treatment of premature ventricular excitation syndromes can be symptomatic (elimination of attacks with medications) or radical (radiofrequency ablation of the abnormal conduction pathway).
Cardiomyopathies
These are myocardial diseases that cause heart failure, not associated with inflammatory processes or pathologies of the coronary arteries.
The most common are hypertrophic and. Hypertrophic is characterized by the growth of the walls of the left ventricle and the interventricular septum, dilated - by an increase in the cavity of the left and sometimes right ventricles. The first is diagnosed in 0.2% of the population. Occurs in athletes and can cause sudden cardiac death. But in this case it is necessary to carry out careful differential diagnosis between hypertrophic cardiomyopathy and non-pathological cardiac enlargement in athletes.

What is meant by congenital heart disease? As a rule, these are defects in any anatomical structure of the heart - septum, valves, great vessels(aorta and pulmonary artery). More than a hundred varieties of congenital heart disease are now known, as well as many of their combinations. Some heart defects are quite common, while others are relatively rare.
Why does congenital heart disease occur?
In the second or third week of pregnancy, the fetus begins to lay various systems, including the heart and great vessels. By the 4th week, when the fetus is only a few millimeters in size, its heart is already beginning to beat. Complete formation of the heart and large vessels of the fetus is completed by the 8th week of pregnancy. The entire cardiovascular system begins to function properly. The occurrence of congenital heart disease is possible if, in the early stages of pregnancy, under the influence of some negative factor, a violation of the correct formation of organs occurs. The following can be considered as such agents that damage the fetus:
- chemicals: varnishes, paints and others
- some medications
- infectious agents (viruses, etc.)
- bad habits of a pregnant woman (smoking, alcohol, substance abuse and drug addiction)
- unfavourable conditions environment(industrial emissions, exhaust gases, radiation, polluted atmosphere)
Particular attention should be paid to the rubella virus. Its affinity for embryonic tissue is well known, which leads to the formation of not only heart defects, but also other congenital anomalies.
It has been reliably determined that in large industrial centers with unfavorable environmental conditions and operating chemical plants, the birth of children with congenital pathologies is higher than, for example, in rural areas.
Hereditary burden cardiovascular pathology, the presence of heart defects in other family members may also play a role.
Sometimes a child is born with a congenital defect, but the cause cannot be determined.
Classification of congenital heart disease
All congenital heart defects, depending on color skin, can be divided into two large groups:
- Blue type, occurring with cyanosis.
- White type, occurring without cyanosis.
Cyanosis (blueness of the skin) is a symptom that occurs due to the mixing of venous and arterial blood.
In relation to the pulmonary circulation, which passes through the lungs, congenital heart diseases are divided into:
- with small circle overload
- with small circle depletion
- without hemodynamic disturbances in the pulmonary circle
Depending on the violation of the anatomical integrity of a particular cardiac structure, congenital heart diseases can be:
- valve
- septal
- combined
With valvular defects, there are abnormalities of the valves. Septal defects imply septal defects; combined congenital defects may include both valve pathology and septal defects or other anomalies.
Main symptoms
Most often, congenital heart disease is diagnosed in the maternity hospital.
The main symptoms are:
- dyspnea
- tachycardia
- heart murmur heard by a doctor
- possible cyanosis or pale skin
- sluggish sucking
With mild congenital heart disease, these manifestations may not occur or they may appear in the child at an older age.
What else might cause concern?
Children with congenital heart disease are often born low birth weight. Sometimes such a child has normal body weight at birth, but then gains weight poorly, developmental delay and malnutrition occurs. Children with congenital heart disease with enrichment of the pulmonary circulation are more likely to suffer from colds, which can be protracted or recurrent; a common acute respiratory infection can develop into bronchitis and pneumonia. It is especially worth being wary when a child often gets sick at an early age and does not attend preschool institutions.
And another cause for concern is the presence of pathological pulsations and the development of deformation of the chest in the area of the heart, the appearance of the so-called cardiac hump.
Children school age sufferers of congenital heart disease may complain of bad feeling, weakness, headaches, dizziness, pain in the heart.
The course of any congenital heart disease is assessed by signs of circulatory failure. These include:
- dyspnea
- tachycardia
- liver enlargement
- swelling
- decreased exercise tolerance
The more pronounced the complex of these manifestations, the greater the degree of circulatory failure and the more severe the defect.
Diagnosis of pathology
Complaints and objective examination data will already allow one to suspect congenital heart disease.
An electrocardiogram will give an idea of the enlargement and overload of certain parts of the heart.
A chest x-ray will show the state of blood flow in the pulmonary circulation, an increase in the shadow of the heart and large vessels.
ECHO-CG (ultrasound of the heart) will determine the specific topic of congenital heart disease, identifying defects in the septa and valves, and assessing the condition of the great vessels.
The most common congenital heart diseases
The most common congenital heart defects are septal defects.
ASD– atrial septal defect, in which there is a pathological communication between the right or left atria, and blood is discharged through it. This is a white type of congenital heart disease with enrichment of the pulmonary circulation. Large atrial septal defects occur with enlargement of the right chambers of the heart, and pulmonary hypertension may develop. Children with ASD are usually born at term, with normal body weight. The systolic heart murmur with this defect is very low-intensity, not rough, and resembles a functional one. Therefore, the diagnosis of the defect is often made after the first year of a child’s life. Children with ASD may often suffer from colds and lag behind in physical development. Atrial septal defects usually require surgical correction. The defect is sutured, large defects are closed with autopericardial or synthetic patches, and endovascular closure using an occluder is increasingly used.
VSD– a defect of the interventricular septum, in which there is a communication between the right and left ventricles with pathological discharge of blood through it. This is a pale type congenital heart disease with enrichment of the pulmonary circulation. There are two varieties of this defect:
- muscle defect
- membranous defect
The muscular defect of the interventricular septum is usually small in size, proceeds favorably, and often tends to spontaneously close. But even if it persists, it does not require surgical correction.
Membranous defects are less favorable. Diagnosed already in the maternity hospital, from 2-3 days of the child’s life a rough blowing systolic murmur in the heart begins to be heard. Children with such defects may lag behind in physical development and often suffer from bronchitis and pneumonia. Large membranous defects require surgical repair. Most often, open heart surgery is performed and a patch is applied to the defect site.
OAP– patent ductus arteriosus (ductus arteriosus). Also very common is congenital heart disease. The ductus botallus during the prenatal period is a normal communication in the fetus and connects the aorta to the pulmonary artery. Patent ductus arteriosus is a vessel through which pathological communication between the aorta and pulmonary artery remains after birth. This is a pale type congenital heart disease with enrichment of the pulmonary circulation. The clinical picture of the defect will depend on the size of the functioning duct. For small sizes it is minimal. With large, wide PDA, it manifests itself at an early age - with audible noise, signs of circulatory failure, the development of malnutrition, and recurrent acute respiratory diseases. The defect is eliminated promptly. The duct is ligated. Now they often resort to an endovascular technique, when an occluder is inserted into the duct to block it.
COARCTATION OF THE AORTA – congenital pathology narrowing of the lumen of the aorta of varying severity anywhere, most often in the area of its isthmus. This heart defect can cause difficulties in diagnosis, since it does not have such a symptom of congenital heart disease as a heart murmur. Sometimes the noise will be heard in the interscapular space from the back. With coarctation of the aorta, the pulsation of peripheral vessels - femoral, popliteal, and dorsum of the foot vessels - is not detected. Symptomatic arterial hypertension develops. Older children have complaints of headaches, nosebleeds, hypertensive crises with high blood pressure, and chilliness of the lower extremities. They have a disproportionate development: well-developed upper shoulder girdle and poorly developed lower limbs. This congenital heart disorder always requires prompt elimination.
AORTIC STENOSIS– white congenital heart disease without hemodynamic disturbances in the pulmonary circulation, when there is an obstruction to the blood flow from the left ventricle to the aorta. There are three types of stenosis: valvular, subvalvular and supravalvular. Valvular aortic stenosis is most common when there is valve deformation. Subvalvular stenosis is characterized by the presence of a membrane or cord narrowing the outflow tract of the left ventricle. Supravalvular stenosis occurs as a result of an obstruction - a fold above the aortic valve. Severe aortic stenosis is eliminated at an early age, minor stenoses long time can be observed conservatively.
PULMONARY ARTERY STENOSIS– white congenital heart disease with depletion of the pulmonary circulation, when there is an obstruction to the flow of blood from the right ventricle to the pulmonary artery. There are two types of defect: valvular and infundibular. With valvular stenosis of the pulmonary artery, fusion of the valve leaflets occurs; infundibular stenosis occurs due to hypertrophy of the outflow tract of the right ventricle or the presence of a septum there. Severe pulmonary artery stenoses are eliminated surgically, minor ones are observed conservatively.
Tetralogy of Fallot– the most common blue heart defect, occurring with the appearance of cyanosis after three months of a child’s life. The tetrad includes four characteristic features: narrowing of the outflow tract of the right ventricle, ventricular septal defect, dextraposition of the aorta (displacement to the right) and hypertrophy of the wall of the right ventricle. Tetralogy of Fallot is eliminated promptly. If previously a series of sequential operations were required, now Tetralogy of Fallot is operated on with one radical surgical intervention.
TRANSPOSITION OF THE GREAT VESSELS, COMMON ARTERIAL TRUNK– severe blue congenital heart disease, manifested by cyanosis from the first hours of the child’s life and requiring emergency cardiac surgery.
Currently, complex, combined congenital heart disease is not uncommon. This is hypoplasia of the left heart, a single ventricle and others.
Treatment methods
The presence of congenital heart disease in a child, as a rule, requires its surgical removal. And it is better to carry out the operation before complications develop: enlargement of the heart, increasing signs of circulatory failure, development of pulmonary hypertension and heart rhythm disturbances. Only a number of defects can be observed conservatively. These include a small muscular defect of the interventricular septum, minor stenosis of the aorta and pulmonary artery.
Some congenital heart defects (they are called critical) must be operated on according to vital signs literally in the first days of a newborn’s life. Such congenital heart defects include transposition of the great vessels, common truncus arteriosus, and pronounced coarctation of the aorta.
Other congenital defects can be operated on in the first years of a child’s life, for example, septal defects, patent ductus arteriosus.
Complex heart defects can be operated on in stages, when a palliative (auxiliary) operation is first performed, and then, when the child’s condition is stabilized, a radical correction of congenital heart disease is performed.
Operations can be performed:
- under conditions of artificial circulation on an open heart
- endovascular method
Endovascular methods for correcting congenital heart disease are now increasingly used. They are performed without an incision in the chest, therefore they are less traumatic and lead to a quick postoperative recovery of the child. These techniques are applicable to the elimination of the most common heart defects, such as atrial septal defect and patent ductus arteriosus.
Prevention of congenital heart disease
Prevention of this pathology in a newborn is aimed, first of all, at eliminating harmful factors. Therefore, we can recommend the following:
- management of a pregnant woman healthy image life
- refusal bad habits
- avoid contact with infectious patients, attending public events during epidemics, rubella vaccination
- avoid occupational hazards for pregnant women and adverse environmental factors (radiation, vibration, chemical agents, etc.)
- acceptance of any medicines during pregnancy only in consultation with a doctor
- reception folic acid during pregnancy planning and in its early stages
- genetic counseling for high risk hereditary pathology, with a history of miscarriages, late pregnancies
Thus, compliance with these simple measures, observation and consultation with a doctor, careful attitude towards yourself, avoidance of harmful factors, especially during the formation of fetal organs and systems, is the key to the birth of a healthy child.
But if a child was born with congenital heart disease, this does not mean a death sentence. Now even the most complex and severe forms are operated on. Pediatric cardiac surgery does not stand still; new techniques are being introduced that spare access to the heart. A timely diagnosis and a successful operation not only save the child, but also return him to a fully fulfilling life!
Heart disease is a disease of the heart valves in which the organ begins to malfunction. As a result of congenital or acquired changes in the structure of the valve apparatus, cardiac septa, walls, or large vessels extending from the heart, a disturbance in the blood flow of the heart occurs. Congenital heart defects are distinguished by a variety of anomalies in the development of the heart and blood vessels and usually appear in childhood. Acquired defects form at different age periods due to heart damage due to rheumatism and some other diseases.
What is the difference between a congenital heart defect and an acquired one?
Congenital heart defect
Congenital heart disease is detected in approximately 1% of newborns. The cause of the disease is improper development of the organ inside the womb. Congenital heart disease affects the walls of the myocardium and large adjacent vessels. The disease may progress. If surgery is not performed, the child may develop changes in the structure of the heart, which in some cases can lead to death. With timely surgical intervention, complete restoration of heart function is possible.
Prerequisites for the development of congenital heart disease:
- developmental disorders of the fetus under the influence pathogenic factors in the first months of pregnancy (radiation, viral infections, vitamin deficiency, uncontrolled intake medicines, including some vitamins);
- parental smoking;
- alcohol consumption by parents.
Acquired heart defect
Acquired heart disease does not occur immediately after birth, but over time. It manifests itself in the form of malfunction of the heart valve apparatus (narrowing of the walls or insufficiency of the heart valves).
Surgical treatment consists of replacing the heart valve with a prosthesis.
If damage to two or more orifices of the heart or valves is detected simultaneously, they speak of a combined acquired defect. To prescribe surgery for an acquired defect, it is classified according to the degree of anatomical changes and disorders.
Causes of acquired heart disease:
Treatment of heart defects
People with heart defects require comprehensive treatment:
- organization of a physical activity regime;
- drug therapy for heart failure and other complications;
- diet;
- physiotherapy.
Surgical treatment is the most effective. Surgical correction is used for both acquired and congenital defects, and operations are increasingly performed on newborns and children from the first year of life.
An acquired defect requires surgical treatment in cases where therapeutic treatment turns out to be ineffective and ordinary physical activity causes fatigue, shortness of breath, palpitations, and angina in patients. Surgeries for acquired defects are performed with the aim of preserving the patient’s own heart valves and restoring their function, including through valvuloplasty (suturing the valves, using animal heart valves, etc.). If valve-sparing surgery is not possible, valves are replaced with mechanical or biological prostheses.
How is heart surgery performed?
Most heart surgeries are performed under artificial circulation. After operations, patients require long-term rehabilitation with a gradual restoration of their physical activity. The deterioration of the operated patient's condition may be associated with the development of complications caused by surgery, so patients should undergo periodic examinations in cardiology centers. With an uncomplicated course postoperative period many patients can return to work 6-12 months after surgery.
* Heart valve - part of the heart formed by its folds inner shell, ensures unidirectional blood flow.
** Myocardium is the middle muscular layer of the heart, constituting the bulk of its mass.
*** Heart valve insufficiency is a type of heart defect in which, due to incomplete closure of the valve, due to its damage, part of the blood flows back to the parts of the heart from which it came.
**** Myocardial infarction - acute form coronary disease hearts.
Acquired heart defects

General information
Acquired heart defects– a group of diseases (stenosis, valve insufficiency, combined and concomitant defects) accompanied by disruption of the structure and functions of the valvular apparatus of the heart, and leading to changes in intracardiac circulation. Compensated heart defects can be secretive; decompensated ones are manifested by shortness of breath, palpitations, fatigue, pain in the heart, and a tendency to faint. If conservative treatment is ineffective, surgery is performed. They are dangerous for the development of heart failure, disability and death.
For heart defects morphological changes heart structures and blood vessels cause disturbances in cardiac function and hemodynamics. There are congenital and acquired heart defects.
In the stage of compensation with slight or moderate mitral valve insufficiency, patients do not complain and do not differ in appearance from healthy people; Blood pressure and pulse were not changed. Mitral heart disease can remain compensated for a long time, however, as the contractility of the myocardium of the left parts of the heart weakens, stagnation increases, first in the pulmonary and then systemic circulation. In the decompensated stage, cyanosis, shortness of breath, palpitations appear, and later - swelling in the lower extremities, painful, enlarged liver, acrocyanosis, swelling of the veins of the neck.
Narrowing of the left atrioventricular orifice (mitral stenosis)
From laboratory studies, the greatest diagnostic value for heart defects, rheumatoid tests, determination of sugar, cholesterol, general clinical blood and urine tests are carried out. Such diagnostics are carried out both during the initial examination of patients with suspected heart disease, and in dispensary groups of patients with an established diagnosis.
Treatment of acquired heart defects
Conservative treatment for heart defects concerns the prevention of complications and relapses of the primary disease (rheumatism, infective endocarditis, etc.), correction of rhythm disturbances and heart failure. All patients with identified heart defects require consultation with a cardiac surgeon to determine the timing of timely surgical treatment.
In case of mitral stenosis, a mitral commissurotomy is performed with the separation of the fused valve leaflets and the expansion of the atrioventricular orifice, as a result of which the stenosis is partially or completely eliminated and severe hemodynamic disorders are eliminated. In case of insufficiency, mitral valve replacement is performed.
In case of aortic stenosis, aortic commissurotomy is performed; in case of insufficiency, aortic valve replacement is performed. In case of combined defects (stenosis of the orifice and valve insufficiency), the destroyed valve is usually replaced with an artificial one; sometimes prosthetics are combined with commissurotomy. In case of combined defects, operations are currently performed for their simultaneous prosthetics.
Forecast
Minor changes in the valvular apparatus of the heart, not accompanied by myocardial damage, can remain in the compensation phase for a long time and not interfere with the patient’s ability to work. The development of decompensation with heart defects and their further prognosis is determined by a number of factors: repeated rheumatic attacks, intoxication, infections, physical overload, nervous strain, and in women - pregnancy and childbirth. Progressive damage to the valve apparatus and heart muscle leads to the development of heart failure, and acute decompensation leads to the death of the patient.
The prognosis for mitral stenosis is unfavorable, since the myocardium of the left atrium is unable to maintain the compensated stage for a long time. With mitral stenosis there is early development pulmonary congestion and circulatory failure.
Prospects for working ability with heart defects are individual and determined by the amount physical activity, the patient’s fitness and condition. In the absence of signs of decompensation, the ability to work may not be impaired; if circulatory failure develops, light work or cessation of work is indicated. For heart defects, moderate physical activity, quitting smoking and alcohol, and performing physical therapy are important. sanatorium treatment at cardiological resorts (Matsesta, Kislovodsk).
Prevention
Measures to prevent the development of acquired heart defects include the prevention of rheumatism, septic conditions, and syphilis. For this purpose, sanitation of infectious foci, hardening, and increasing the body's fitness are carried out.
In case of established heart disease, in order to prevent heart failure, patients are advised to follow a rational motor regimen (walking, physiotherapy), complete protein nutrition, restriction of intake table salt, abandon sudden climate changes (especially high-altitude ones) and active sports training.
In order to control the activity of the rheumatic process and compensate for cardiac activity in case of heart defects, it is necessary dispensary observation at the cardiologist.