The popliteal artery is a fairly large vessel that directly continues downwards. It lies within the neurovascular bundle, together with the vein of the same name and the tibial nerve. At the back, on the side of the popliteal fossa, the vein lies closer to the surface than the artery; and the tibial nerve is even more superficial than blood vessels.
Location and topography
Beginning at the lower aperture of the adductor canal, located under the semimembrane of mice, the popliteal artery is adjacent at the bottom of the popliteal fossa, first to the femur (directly to the popliteal surface), and then to the capsular membrane knee joint.
The lower part of the artery is in contact with It penetrates the narrow space between the bellies of the gastrocnemius muscle, which cover it. And having reached the edge of the soleus muscle, the vessel divides into the posterior and anterior tibial arteries.

The direction of the popliteal artery changes along its length:
. IN upper section the popliteal fossa, the vessel has a downward and outward direction.
. Starting from the level of the middle of the popliteal fossa, the popliteal artery is directed almost vertically downwards.
Branches of the popliteal artery
Along its length, the popliteal artery gives off a number of branches:
. Upper muscular branches.
. Superior lateral genicular artery.
. Superior medial genicular artery.
. Middle genicular artery.
. Inferior lateral genicular artery.
. Inferior medial genicular artery.
. Calf arteries (two; less often - more).
Popliteal artery aneurysm
According to medical statistics, this is the most common location of aneurysms in the periphery: about 70% of peripheral aneurysms are localized in the popliteal region. The main reason for this pathological condition atherosclerosis is generally considered to be the cause, since it is established as an etiological factor in the vast majority of patients with popliteal artery aneurysm.
Popliteal artery aneurysm develops almost regardless of age; average age The patients are approximately 60 years old, and the age range is from 40 to 90 years. Bilateral lesions are recorded in 50% of cases.
Much more often this disease affects men.
IN clinical picture symptoms of ischemic damage predominate distal section limbs; Symptoms of compression of the nerve and vein (when they are compressed by an aneurysm) may also be added.
Complications:
. thrombosis of aneurysm (aneurysmal cavity);
. aneurysm rupture;
. calcification of the aneurysm;
. nerve compression.
For diagnostics the following are used:
. angiography;
. CT scan.
For treatment, ligation of the popliteal artery on both sides of the aneurysm (proximal and distal to it) is most often performed, followed by bypass surgery.
Thrombosis of the popliteal artery

A predisposing factor for the formation of blood clots in the arteries is damage to the inner surface of the vessels, the causes of which may be the following factors:
. atherosclerotic deposits on the walls of blood vessels;
. hypertonic disease;
. diabetes;
. traumatization vascular wall;
. vasculitis
Clinical manifestations
Thrombosis of the popliteal artery is manifested by the following symptoms:
. Severe pain in the limb, appearing suddenly. Patients often compare its appearance to a blow. In the future, the pain may become paroxysmal; Moreover, an attack of pain leads to the appearance of sweat on the skin. Some reduction in pain over time does not mean an objective improvement in the patient’s condition.
. Pallor of the skin of the affected limb.
. Decreased skin temperature of the affected limb.
. The appearance of a thickening on the leg; its location coincides with the level of localization of the thrombus.
. Decreased and later disappearance of sensation in the leg; the appearance of paresthesia.
. Restricted mobility of the affected limb. In the future, mobility may be completely lost.
As a rule, symptoms develop gradually, starting with the onset of pain.
In the absence of adequate measures, a complication in the form of gangrene may develop. This condition is characterized by the presence of a clear boundary between normal and necrotic tissue. Subsequently, the necrotic area is mummified.
The worst case scenario is infection of the necrotic area. This condition is diagnosed by rapidly developing hyperthermia, pronounced leukocytosis in the blood and the presence of ulcerative decay.
popliteal artery,a. poplitea (Fig. 64), is a continuation of the femoral artery. At the level of the lower edge of the popliteus muscle, it is divided into its terminal branches - the anterior and posterior tibial arteries. Branches of the popliteal artery:
1 Lateral superior genicular artery, a. genus superior lateralis [ a. superior lateralis genus], It departs above the lateral condyle of the femur, goes around it, supplies the vastus and biceps femoris muscles and anastomoses with other knee arteries, participating in the formation of the knee articular network that supplies the knee joint.
2 Medial superior genicular artery, a. genus superior medialis [ a. superior medialis genus], departs from the popliteal artery at the same level as the previous one, goes around the medial condyle of the femur, supplies blood to the vastus medialis muscle.
3 Middle genicular artery, a. media genus, goes to back wall the capsule of the knee joint, to its cruciate ligaments and menisci, supplies them and the synovial folds of the capsule with blood.
4 Lateral inferior genicular artery, a. genus inferior lateralis [ a. inferior lateralis genus], departs from the popliteal artery 3-4 cm distal to the superior lateral knee artery, goes around the lateral condyle of the tibia, supplies the lateral head of the gastrocnemius muscle and the plantaris muscle.
5 Medial inferior genicular artery, a. genus inferior medialis [ a. inferior medialis genus], originates at the level of the previous one, goes around the medial condyle of the tibia, supplies the medial head of the gastrocnemius muscle and also participates in the formation knee joint network,rete articuldre genus.
108. Arteries of the leg: topography, branches and areas supplied by them. Blood supply to the ankle joint.
Posterior tibial artery,a. tibidlis posterior, serves as a continuation of the popliteal artery, passes through the ankle-popliteal canal, which leaves under the medial edge of the soleus muscle. Then the artery deviates to the medial side, goes to the medial malleolus, behind which in a separate fibrous canal under the retinaculum of the flexor tendons it passes to the sole. At this point, the posterior tibial artery is covered only by fascia and skin.
Branches of the posterior tibial artery:
1. Muscle branches,rr. musculares, - to the muscles of the lower leg;
2. Branch circumflexing the fibulaG.circumflexus fibuldris, departs from the posterior tibial artery at its very beginning, goes to the head of the fibula, supplies blood to the adjacent muscles and anastomoses with the knee arteries.
3. peroneal artery,A. regopea [fibuldris], follows laterally, under the flexor longus thumb foot (adjacent to the fibula), then down and penetrates the lower musculofibular canal. Passing along the posterior surface between the bone membrane of the leg, it supplies blood to the triceps muscle of the leg, the long and short peroneus muscles and behind the lateral malleolus of the fibula it is divided into its terminal branches: lateral ankle branches,rr. malleolares laterales, And calcaneal branches,rr. calcdnei, involved in education heel net,rete calcaneum. The peroneal artery also gives off perforating branch, Mr.perforans, anastomosing with the lateral anterior malleolar artery (from the anterior tibial artery), and connecting branch, sosh-municans, connecting the peroneal artery with the posterior tibial artery in the lower third of the leg.
4Medial plantar artery,a. plantdris medialis (Fig. 65), - one of the terminal branches of the posterior tibial artery. It passes under the abductor hallucis muscle and lies in the medial groove of the sole, where it divides into superficial and deep branches,rr. superficidlis et profundus. The superficial branch feeds the abductor hallucis muscle, and the deep branch supplies the same muscle and the flexor digitorum brevis. The medial plantar artery anastomoses with the first dorsal metatarsal artery.
5Lateral plantar artery,a. plantdris lateralis, larger than the previous one, runs in the lateral groove of the sole to the base of the fifth metatarsal bone, bends in the medial direction and forms at the level of the base metatarsal bones [deep] plantar arch,drcus plantdris [ profundus] (see Fig. 71). The arch ends at the lateral edge of the first metatarsal bone with an anastomosis with the deep plantar artery - a branch of the dorsal artery of the foot, as well as with the medial plantar artery. The lateral plantar artery gives branches to the muscles, bones and ligaments of the foot.
Four branches extend from the plantar arch plantar metatarsal arteries, aa.metatdrsales plant trees I-IV. The perforating branches of the dorsal metatarsal arteries flow into these arteries in the interosseous spaces. The plantar metatarsal arteries, in turn, give off perforating branches,rr. perfordntes, to the dorsal metatarsal arteries.
Each plantar metatarsal artery passes into common plantar digital artery,a. digitalis plantdris com- munis. At the level of the main phalanges of the fingers, each common plantar digital artery (except the first) is divided into two own plantar digital arteries, aa.digits plan tdres propriae. The first common plantar digital artery branches into three own plantar digital arteries: to the two sides of the big toe and to the medial side of the second finger, and the second, third and fourth arteries supply blood to the sides of the second, third, fourth and fifth fingers facing each other. At the level of the heads of the metatarsal bones, perforating branches are separated from the common plantar digital arteries to the dorsal digital arteries.
Anterior tibial artery,a. tibialis anterior, departs from the popliteal artery in the popliteal fossa (at the lower edge of the popliteal muscle), enters the ankle-popliteal canal and immediately leaves it through the anterior opening in the upper part of the interosseous membrane of the leg. Then the artery descends along the anterior surface of the membrane and continues onto the foot as the dorsal artery of the foot (Fig. 66).
Branches of the anterior tibial artery:
1Muscular branchesrr. musculares, to the muscles of the lower leg.
2Posterior tibial recurrent artery,A. gesig-rens tibialis posterior, departs within the popliteal fossa, anastomoses with the medial inferior knee artery, participates in the formation of the knee articular network, supplies blood to the knee joint and popliteal muscle.
3Anterior tibial recurrent artery,A. gesig-rens tibialis anterior, originates from the anterior tibial artery as it exits the anterior surface of the leg, goes upward and anastomoses with the arteries that form the knee articular network. Takes part in the blood supply to the knee and tibiofibular joints, as well as the tibialis anterior muscle and extensor digitorum longus.
4Lateral anterior malleolar artery,a. malleold- ris anterior lateralis, begins above the lateral malleolus, supplies blood to the lateral malleolus, ankle joint and tarsal bones, takes part in the formation lateral ankle network,rete malleoldre later, anastomoses with the lateral ankle branches (from the peroneal artery).
5Medial anterior malleolar artery,a. malleold- ris anterior medlis, departs from the anterior tibial artery at the level of the previous one, sends branches to the capsule of the ankle joint and anastomoses with the medial ankle branches (from the posterior tibial artery), participates in the formation of the medial ankle network.
6Dorsal artery of the foot,a. dorsdlis pedis (continuation of the anterior tibial artery), runs anterior to the ankle joint between the tendons of the long extensor digitorum in a separate fibrous canal. At this point, the artery lies under the skin and is accessible to determine the pulse. On the dorsum of the foot it goes to the first interosseous space, where it divides into terminal branches: 1) the first dorsal metatarsal artery, a. metatarsdlis dorsdlis I, from which three depart digits dorsdles, to both sides of the dorsum of the thumb and the medial side of the second finger; 2) deep plantar branch [artery], a. plantdris profunda, which passes through the first intermetatarsal space onto the sole, piercing the first dorsal interosseous muscle, and anastomoses with the plantar arch. The dorsal artery of the foot also gives off the pretarsal arteries - lateral and medial, ah.tarsdles laterlis et medlis, to the lateral and medial edges of the foot and the arcuate artery, A. ag-cudta, located at the level of the metatarsophalangeal joints and anastomosing with the lateral metatarsal artery. I-IV extend from the arcuate artery towards the fingers dorsal metatarsal arteries, aa.metatdrsales dorsdles I-IV (see Fig. 66), each of which is divided into two at the beginning of the interdigital space dorsal digital arteries, aa.digits dor sdles, heading towards the backs of adjacent fingers. From each of the dorsal digital arteries, perforating branches extend through the intermetatarsal spaces to the plantar metatarsal arteries.
For the arteries of the pelvis and lower limb characterized by the presence of anastomoses between the branches of the iliac, femoral, popliteal and tibial arteries, which provide collateral flow of arterial blood and blood supply to the joints (Table 5). On the plantar surface of the foot, as a result of the anastomosis of the arteries, there are two arterial arches. One of them - the plantar arch - lies in the horizontal plane. It is formed by the terminal section of the lateral plantar artery and the medial plantar artery (both from the posterior tibial artery). The second arc is located in the vertical plane; it is formed by an anastomosis between the deep plantar arch and the deep plantar artery - a branch of the dorsal artery of the foot. The presence of these anastomoses ensures the passage of blood to the toes in any position of the foot.
Popliteal artery a. Popliteal is responsible for the blood supply to the muscles of the leg and knee joint. All branches widely entwine the leg, connecting with each other, thus forming a single vascular network. It arises from the femoral artery and, when passing through the popliteal fossa, is tightly pressed against the bone when the leg is bent. Then it passes through the joint capsule of the knee and rushes down almost vertically. A vein runs parallel along the artery, which has the same name, as well as the tibial nerve.
As it runs, the popliteal artery branches into a large number of branches, which in turn also branch, creating a single network, the purpose of which is to supply blood to all components of the legs.
Aneurysm a. Popliteal
The word “aneurysm” refers to a limited or diffuse increase in the lumen of a blood vessel. That is, the formation of a local protrusion in some part of the vessel. The shape of such a formation is similar to a sac, which is why it received another name - saccular aneurysm.
In one case out of five, aneurysms occur during plural. The size of the formation in most does not exceed 1 cm, but in some cases it can increase two or even three times. In the latter case, they are called giant. 
Symptoms
Symptoms of a popliteal artery aneurysm are the appearance of a protruding formation that has a tumor-like shape. In this case, the patient feels pulsation at the site of formation, along with acute pain, which gradually recedes over time.
Symptoms also include the patient feeling of weakness in the limb on which the formation appeared; numbness and decreased sensitivity in the leg are possible. External symptoms, in addition to the appearance of the formation itself, include pallor skin feet and cold feet.
To prevent diseases and treat manifestations of varicose veins on the legs, our readers recommend Anti-varicose gel "VariStop", filled with plant extracts and oils, it gently and effectively eliminates the manifestations of the disease, alleviates symptoms, tones, and strengthens blood vessels.
Doctors' opinion...
Risk group and prognosis for disease development without intervention
More often develops in older people suffering long time hypertension and smoking abusers. In addition, the development of the disease is facilitated by the presence of vasculitis, injuries with subsequent vascular dysfunction, and atherosclerotic lesions. In addition, people who prefer a diet with a large amount of animal fats are more susceptible to the disease.
The prognosis for the development of the disease without medical intervention is negative. Such formations can lead to tragic consequences, such as acute ischemia due to aneurysm rupture, acute arterial insufficiency, thrombosis with further occlusion of the popliteal artery. In addition, gangrene may develop, first in the nearest tissues, and then in the entire leg. 
Treatment
Treatment of an aneurysm is carried out in two ways: open and surgical non-open surgery. Open intervention involves surgery on a vessel by a vascular doctor. It consists of obtaining open access to the popliteal artery by dissecting the tissue of the affected area and the artery at the site of the identified formation. For bypass surgery, either a similar vessel, which is extracted from the patient’s body, or an artificial implant can be used.
With a closed intervention, a minimally invasive procedure is used, which consists of installing a stent on the affected area of the popliteal artery by inserting a catheter.
Thrombosis a. Popliteal
Popliteal artery thrombosis is the obstruction of an artery due to a blood clot. Vessel obstruction can be determined quite accurately by certain symptoms. So, if a patient complains of leg pain in a supine position, and at the same time painful sensations in the latter, they decrease when sitting on a chair, or lowering one’s leg from the bed, then it can be assumed that thrombosis is developing. But such clinical data cannot be taken as complete confirmation of the disease. Used for precise localization of thrombus instrumental diagnostics in the form of arteriography. 
The course of the disease occurs quickly. First, the patient notices a gradually increasing pain in the legs when walking. As the clot grows, the lumen gradually decreases, which leads to insufficient nutrition of the limb. The patient's skin sensitivity begins to decrease and becomes pale. Then the beating of the vessel in the lower part from the thrombus ceases to be heard. Over time, the pain increases, and the skin first turns purple and then black. Then gangrene of the limb begins.
Treatment
Thrombosis is treated by a vascular surgeon. Intervention must be urgent, since the development of the disease occurs quite quickly and can lead to dire consequences in the form of gangrene of the limb. The attending physician decides to hospitalize the patient and prepare him for surgery. At the same time, the patient is prescribed painkillers and vasodilators.
At surgical intervention access to the popliteal artery is carried out from the medial side or posteriorly. The medial side in this case is more preferable, since it allows you to bypass sciatic nerve, which is not possible with rear access.
Once access is obtained, the artery is incised in the area of the thrombus and endarterectomy is performed, after which a venous patch is performed at the site of obstruction.
Rice. 793. Arteries of the gluteus medius muscle, right (X-ray photograph. Preparation by N. Rybakina). (The largest vessels in the thickness of the muscle are presented.)
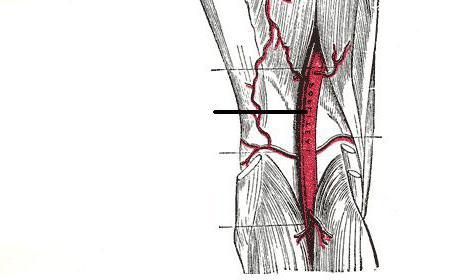
Popliteal artery, a. poplitea (Fig. , , , ; see Fig. , , ), is a direct continuation of the femoral artery. It begins at the level of the lower opening of the adductor canal, lies under the semimembranosus muscle and runs along the bottom of the popliteal fossa, adjacent first to the popliteal surface of the femur and then to the articular capsule of the knee joint, and in its lower part to the popliteal muscle. The popliteal artery is directed first down and somewhat laterally, and from the middle of the popliteal fossa it is almost vertical.
The lower part of the artery passes into the gap between the heads of the gastrocnemius muscle covering it, and at the level of the lower edge of the popliteus muscle, the artery follows between it and the heads of the gastrocnemius muscle; under the edge of the soleus muscle it divides into the posterior tibial artery, a. tibialis posterior, and anterior tibial artery, a. tibialis anterior.
The popliteal artery is accompanied throughout its entire length by the vein of the same name and the tibial nerve, n. tibialis. On the side of the popliteal fossa, behind, the vein lies superficially, and the nerve lies even more superficially in relation to the artery and vein.
Along its course, the popliteal artery gives off a number of branches that supply blood to the muscles and knee joint. All these branches widely anastomose with each other, as well as with the rr. perforantes (branches of a. profunda femoris) and a. descendens genicularis (branch of A. femoralis), forming a dense vascular knee articular network (see Fig.).
A number of branches depart from the popliteal artery (see Fig.,).
- Lateral superior genicular artery, a. superior lateralis genus, goes outward under the biceps femoris muscle and, heading over the lateral condyle, breaks up into smaller branches that take part in the formation of the knee articular network.
- Medial superior genicular artery, a. superior medialis genus, is directed anteriorly under the tendons of the semimembranosus and adductor magnus muscles, above the medial condyle and, bending around with inside femur, takes part in the formation of the knee joint network.
- Middle genicular artery, a. media genus, directed from the popliteal artery anteriorly, above the oblique popliteal ligament, it pierces the capsule of the knee joint and gives off a number of branches to the synovial membrane of the joint and the cruciate ligaments.
- Lateral inferior genicular artery, a. inferior lateralis genus, starts from the most distal part of the popliteal artery, passes under the lateral head of the gastrocnemius muscle and the biceps femoris muscle, bends around the knee joint above the head of the fibula and, emerging on the anterior surface of the knee, takes part in the formation of the knee joint network.
- Medial inferior genicular artery, a. inferior medialis genus, passes under the medial head of the gastrocnemius muscle and goes around the medial periphery of the knee joint, lying under the tibial collateral ligament. The branches of the artery are part of the network of the knee joint.
- Calf arteries, aa. surales, only two (sometimes more), arise from the posterior surface of the popliteal artery and, breaking up into a number of smaller branches, supply blood to the proximal parts of the triceps and plantar muscles of the leg and the skin of the leg.
The heart and blood vessels function normally when all arteries are in a healthy state. They entangle human organs with their networks and solve one problem - to ensure long-term functioning of the heart and the body as a whole.
The arterial network of the knee joint can withstand intense blood flow, so it must be strong and reliable. The work of the legs, spine, and organs connected to the legs through networks depends on blood circulation. Slowing down the flow of blood in the artery or blocking it with blood clots or fat bubbles causes diseases.
Functional purpose of the network of arteries under the knee
Arteries of the lower extremities
In the circulatory system, the popliteal artery continues the network of femoral arteries, which, under the knee, is divided into final branches - anterior and posterior vessels. This forms the knee arterial network, which weaves around the lower leg and foot.
Functions of arteries:
- The lateral superior solves the problem of blood supply to the thigh muscles: the vastus and biceps.
- The medial superior blood supply to the thigh muscle, which in the topography of the arterial network is called broad, is located closer to the median plane of the leg.
- The middle one solves the problem of blood supply to the ligaments, menisci, synovium, and capsular component.
- The lateral inferior provides blood supply to the calf and plantar muscles.
- The medial inferior supplies blood calf muscles, is an integral part of the branches of the popliteal artery.
- The posterior tibial continues the anatomy of the popliteal artery, is located in a special canal under the knee, where the arteries and veins go, and supplies blood to the muscles of the lower leg.
Branches of the arteries of the tibia under the leg:
- Muscle branches directed to the ankle.
- The branch around the fibula supplies blood to the adjacent muscles.
- The peroneal vessels supply blood to the triceps, long and short muscles. Here the network is distributed into terminal branches running along the ankle and heel and entwining the heel.
- The medial plantar branches into superficial and deep vessels. The superficial network entangles the adductor muscle thumb legs, the deep one also nourishes the short muscles that flex the fingers.
- The lateral plantar on topography looks like an arch of the sole extending into the base of the metatarsal bones. The branches entangle the muscles, bones, and ligaments of the foot.
This ensures adequate blood supply to all parts of the lower leg. This is important for normal functioning and to withstand the load that falls on your legs during the day. The knee is supplied by a network of blood vessels that branches off from the anterior tibial artery.
Collaterals in the structure of the knee joint
 The collateral connection in the circulatory system under the knees is a special network that has a complex structure in supplying blood to the leg from the knee to the foot. The popliteal arteries depart from the femoral condyles to the knee joint and pass into its upper blood vessels. The branching in front on the surface of the leg forms an anastomosis with the vessels on the lower leg and their branches.
The collateral connection in the circulatory system under the knees is a special network that has a complex structure in supplying blood to the leg from the knee to the foot. The popliteal arteries depart from the femoral condyles to the knee joint and pass into its upper blood vessels. The branching in front on the surface of the leg forms an anastomosis with the vessels on the lower leg and their branches.
The scheme of collateral connections in the structure of the knee joint includes anastomosis lower arteries- paired vessels extending from the popliteal arteries to the superior paired vessels - they make up the arterial network. The network in its distal part necessarily includes the arteries of the lower leg, which give off a return branch that connects with the permanent return artery.
When it is necessary to ligate the popliteal artery, the collateral network is the connection of the vessels of the thigh and leg. The artificial creation of blood circulation by collateral route distributes the switched off branches, if required by treatment after a disease or injury.
Arterial component of blood supply
The blood supply to the knee joints is provided by arterial networks parallel to both legs. A special task is solved by the middle artery of the knee, which is tasked with feeding the internal structures of the joint - menisci, synovial tissue, cruciate ligaments.
Descending arteries stretch from the femoral vessels to the knee vessels, and two return arteries from the tibial vessels. The outflow of blood is provided by veins with the same names. All of them are topographically located in areas of the joint capsule where the least compression is provided, so that blood supply in both directions is carried out at a normal speed.
The functions of the legs depend on the normal functions and integrity of the network of popliteal arteries. If, as a result of a knee injury, an artery ruptures, open or closed, it is accompanied by hemorrhage, which cuts off the nutrition of all leg muscles and all structures of the knee joint. If a hematoma appears on the knee, pain and limping, you should consult a doctor.
Are used simple methods research – external definition gait, examination of the knee with the patient lying on his back, palpation of the knee joint, determination of the condition of the subcutaneous vascular network. When palpating the hematoma, its depth and the possibility of penetration into the internal structures of the knee are determined.
Impaired blood supply due to injury or disease leads to atrophy of the muscles of the thigh, leg, and foot. This is determined visually and by measuring the topography of knee motion.
Treatment of pathologies of the arterial system
 Damage is the most common form of pathology circulatory system legs These are open cuts, tissue tears due to serious injury, or closed injuries from blows, bruises, sprains. Knee bruises are accompanied by internal hemorrhage and damage to the periarticular tissues.
Damage is the most common form of pathology circulatory system legs These are open cuts, tissue tears due to serious injury, or closed injuries from blows, bruises, sprains. Knee bruises are accompanied by internal hemorrhage and damage to the periarticular tissues.
Home treatment for minor injuries: apply a pressure bandage, apply a cold compress, relieve the sore leg as much as possible. After 2-3 days, you can apply warming compresses, take warm baths, UHF procedures, and exercise therapy.
During the course of hemarthrosis, hemorrhage occurs in the internal cavity of the joint, the synovial membrane is damaged, and its vessels rupture. A puncture is necessary to remove blood from the internal space of the joint and inject a 20 ml solution of novocaine into 20 ml. After this, a plaster splint is applied to the affected leg for a week. Next, the doctor prescribes UHF, electrophoresis, and exercise therapy. Restoration of the functions of the circulatory system occurs within a month.

